 Translate
Translate





A Health Impact Assessment Of Health, Equity And Social Impacts
Table of Contents
- Contributions
- Executive Summary
- Introduction
- Baseline Conditions
- Assessment
- Recommendations
- Addendum
- Endnotes
- Appendices
Contributions
Authors
Clackamas County Public Health Division (CCPHD)
- Abe Moland, MPH, MURP (former)
- Jamie Zentner, MPH
- Molly Mew, MPH
- Marc Czornij
- Kate Marsi, MPH (former)
Acknowledgements
We wish to thank the following stakeholders for their collaboration and engagement in conversations around cannabis policy in the county:
- Erin Zumbaum
Amberlight Cannabis House - Brad Troutner
Cannabis Agricultural Business Park - Casey Palmer
Mary Rumbaugh
CC Behavioral Health - Brian McCrady
CC Children, Family, Community Connections - Brian Imdieke
CC Community Corrections - Kathleen Rastetter
CC County Counsel - Jennifer Hughes
Joe Marek
Rob Sadowsky
CC DTD - Jon Legarza
CC Economic Development - Andrew Suchocki
CC Health Centers - Allison Coe
Jemila Hart
CC Housing Authority - Katie Anderson
CC Juvenile Department - Kathryn Kohl
CC Libraries - Rick Gruen
CC Parks and Forest - Graham Phalen
CC Sheriff’s Office - Brenda Durbin
CC Social Services - Samara Phelps
CC Tourism & Cultural Affairs - Jason Wach
City of Milwaukie - Dan Huff
City of Molalla - Michelle Veenker
NAMI - Zeenia Junkeer
OHEA - Jana Lombardi
Stafford Hamlet Board - Mike Turley
Stone Creek Golf Course
We also thank the colleagues and partners who provided valuable feedback on this report:
- Bryan Hockaday
CC Public and Government Affairs - Kamryn Brown
Marco Enciso
Katie Knutsen
Kim LaCroix
Phillip Mason-Joyner
Chijioke Oranye
Dr. Sarah Present
Erika Zoller
CCPHD - Emily Droge
Tara Weston
Oregon Health Authority
The views expressed in this report do not necessarily reflect the official policies or perspectives of Clackamas County or partner organizations.
Executive Summary
Evaluating Impacts of State Public Consumption of Cannabis in Clackamas County
Public consumption of cannabis is currently illegal in Oregon. Instead, the State’s legalization policy permits cannabis use in private residences only. Cannabis advocates argue that this creates inequities in access for people living in rental housing, specifically low-income renters, who do not have access to private space (such as a backyard, patio, or owned residence) where cannabis is allowed. Furthermore, the repercussions for illegal public consumption of cannabis have fallen disproportionately on communities of color through over policing and racial profiling practices.
Policies that allow consumption of cannabis at public venues are seen as a possible solution to these issues, but also come with trade-offs. Places where public consumption is allowed, either indoors or outdoors, expose more people to secondhand cannabis smoke, normalizes use among youth, and increases the likelihood someone may drive under the influence of cannabis traveling to and from these locations. Due to the novelty of this policy, there is limited information on which to develop an evidence-based position.
This health impact assessment (HIA) evaluates the question “What are the health, social and equity implications of public consumption of cannabis in Clackamas County?” to proactively address an emerging public health issue while building a practice of evidence-based policy making. Recommendations have been crafted based on findings from this assessment, which include:

A policy scan of relevant local, state and national practices related to public consumption of cannabis and a literature and data review of linked health outcomes.

24 stakeholder interviews across multiple sectors in Clackamas County gauging concerns related to public consumption policy and thoughts on mitigations.

A framing analysis to distill core perspectives and talking points of 85 public testimonies submitted on House Bills containing public consumption of cannabis policy.
Legislative Takeaways
In the 2019 and 2021 Oregon legislative sessions, bills proposing the lawful consumption of cannabis in various formats and venues of public consumption were introduced. These have included allowing public consumption at cannabis cafes, cannabis farm tastings, and permitting consumption at temporary events and licensed cannabis retail locations. The notable difference between 2019 and 2021 was the form cannabis could be consumed. All forms of consumption were allowed in 2019; smoking and vaping were not allowed indoors in 2021.
HB 2233 & SB 639 (2019)
- Legalizing cannabis consumption cafes to:
- Allow retailers to add all forms of tasting and consumption spaces to their businesses
- Allow stand-alone cafes where consumers can share their own cannabis products
- Create temporary event licenses that allow for regulated cannabis consumption spaces at public events
- Create opportunities for farm tourism that allows for sales and consumption to occur on licensed cannabis farms, emulating the winery model and bringing a new revenue stream for licensed farmers
- Allow for new business models such as cannabis spas and bud and breakfasts, and create opportunities for more business development and more tourism dollars to flow into Oregon
- Expand deliveries to participating hotels and temporary residences
HB 3112 (2021)
- Provision of free, automatic expungement of qualifying cannabis crimes
- Investment of cannabis tax dollars into BIPOC businesses, to programs focused on land ownership, job training, wealth creation, and reducing racial disparities in education outcomes
- Creation of an Equity Investment Governing Board to provide equity oversight for the state
- Creation of equity licenses to support BIPOC cannabis business owners that would include:
- License fee reduction and dedicated staff at OLCC to support processing times
- Provision of capital and technical support to address funding and resource inequities
- On premise consumption (smoking and vaping prohibited indoors) and expanded delivery licenses exclusive to equity licenses for a period of ten years
During both sessions, a majority testimony was submitted in support of the bills. However, because the policy levers within each bill were significantly different, the stakeholders, conversations and concerns shifted between sessions:
- Stakeholders. During the session for HB 2233, testimony came from cannabis businesses, citizens, government agencies, and community based and health advocacy groups. During the session for HB 3112, testimony was largely submitted from lawyers and academic institutions, as well as the same stakeholders for HB 2233. Fewer health advocacy groups testified in HB 3112. This may have been a product of the COVID-19 pandemic, which limited participation from the health field.
- Conversations. Testimonies in support of HB 3112 reflected the leading issues in the bill that centered racial equity and justice verses HB 2233 that focused on the consumption of cannabis at public events and venues. Frames around equity almost entirely shifted to center communities of color in HB 3112 as opposed to low-income renters in HB 2233.
- Concerns. Despite the increase in the overall amount of testimony submitted between sessions, the oppositional testimony decreased by almost 50% during the 2021 session. Fewer people brought up the risks of public consumption of cannabis associated with driving under the influence of cannabis, impacts to youth and mental health, and exposure to secondhand smoke since smoking and vaping were not permitted. The opposition instead shifted to application of the racial equity lens.
Stakeholder Interview Findings
The stakeholders interviewed in 2019 for this HIA represented a wide range of sectors that intersect with cannabis and provide varied perspectives. They noted present concerns of current cannabis consumption related to mental health, including disproportionate impacts on youth and the potential to worsen certain conditions, such as depression and anxiety. Current use as a gateway to using other substances was also mentioned by several participants. Some stakeholders shared they did not have any present concerns regarding cannabis impacting their sector.
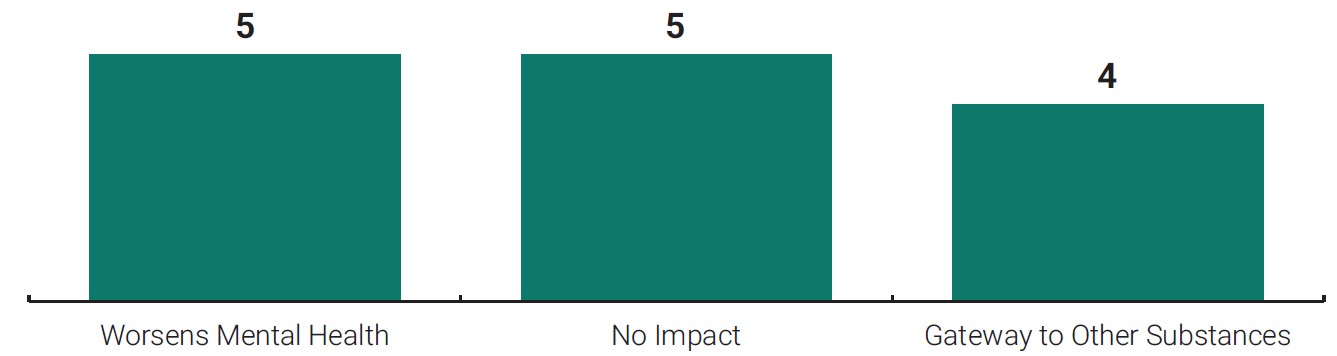
Figure 1. Stakeholders’ Top Present Concerns of Cannabis Use
- Worsens mental health: 5
- No impact: 5
- Gateway to other substances: 4
Stakeholders thought public consumption policy would increase normalization, decrease road safety, and increase use.
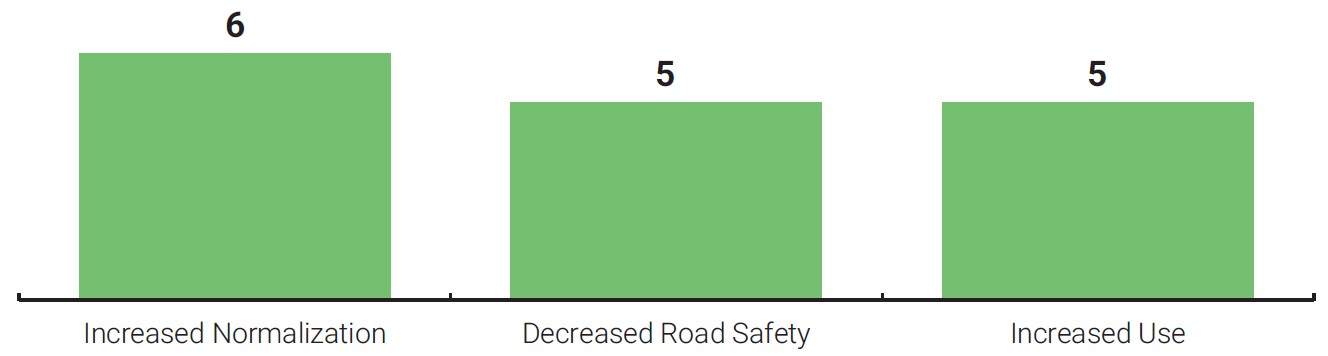
Figure 2. Stakeholders’ Top Future Short-Term Concerns of Public Consumption Policy
- Increased normalization: 6
- Decreased road safety: 5
- Increased use: 5
Anticipated Impacts
Based on stakeholder interviews, legislative conversations and best available evidence, below is a summary of the possible impacts in Clackamas County from a state public consumption policy. Because of the novel nature of public consumption, additional unanticipated impacts are possible.
Health
- A consumption policy that allows the public smoking of cannabis poses an environmental health threat to neighboring residents and employees at public consumption sites. There is no level of safe exposure to primary or secondhand smoke.
- Based on the rural nature of the county, public consumption locations are likely to be dispersed. This would require visitors to reach them using a personal vehicle, which could increase instances of driving under the influence and thus threaten the safety of pedestrians and other road users.
- Heavy cannabis use is connected to risk of worsening mental health conditions. Increasing access and normalization of cannabis in the county could complicate and worsen mental health trends.
Social
- The creation of destinations for public consumption of cannabis will have local, site-specific impacts in both urban and rural areas that will affect safety and livability.
- Rates of cannabis use by Clackamas County youth have held steady over the past years, while Oregon has seen increases in adult use. It is possible that youth use would increase through increased marketing exposure and normalization.
- Cannabis-related employment and tax revenue are likely to increase because of new sales opportunities.
Equity
- Leading with racial equity in the development of a public consumption policy can address past harms and support equitable distribution of economic benefits in the county.
- Additional work is needed to build stakeholder capacity to ensure health outcomes and cannabis access are not uneven in the county.
Recommendations
Decision makers should consider the full range of health risks and benefits of public consumption of cannabis. If public consumption policy is passed, the following recommendations offer strategies to mitigate potential harms and maximize benefits to improve health equity throughout Clackamas County:
- Support and increase health equity-focused advocacy in cannabis policy development as legislation is being shaped. There was a lack of health-focused advocacy in the 2021 legislative session. State policy should cite and account for related health disparities and associated determinants.
- Adopt local regulations and zoning requirements to reduce the impact of public consumption of cannabis on neighborhood health. Health-promoting policies need to intentionally shape the indoor and outdoor built environment to support healthy communities.
- Establish an equity lens to guide the development and evaluation of cannabis use and regulation. Policies should consider communities disproportionately and negatively impacted by issues associated with substance use and other related health harms. The topic of equity was notably absent in Clackamas County stakeholder interviews, with concerns about disproportionate impacts only surfacing in three of 24 interviews.
- Dedicate funding and resources for systems to promote safety and limit driving under the influence of cannabis. Creating public consumption spaces induces a need for travel. Current land use and zoning make driving the easy choice. Given the already growing number of crashes involving some form of substance, additional safety efforts are needed.
- Develop public information materials on lower risk cannabis use, cannabis consumption types and the impacts of secondhand cannabis smoke exposure. As cannabis normalization and use continue to grow, so too must related health and safety education and awareness efforts.
- Create strong accountability mechanisms to ensure benefits to historically marginalized groups are maintained for the lifespan of public consumption policy. Past renditions of policies have had limited evaluation components to ensure disparities are being reduced.
- Advocate for the use of cannabis tax revenue for local interventions to support livability and reduce unintended impacts on the surrounding area. Neighborhoods with higher densities of low-income and BIPOC communities are at risk of being disproportionately saturated with venues allowing public consumption.
- Establish partnerships with local researchers to translate evidence to policies, systems, and environments that promote healthy communities and advocate for research in rural settings. Research on the relationship between cannabis use and health outcomes is limited. Establishing relationships with local research partners is key to developing relevant and actionable evidence.
Introduction
Cannabis is classified as illegal in the United States under federal law, but the policy landscape is rapidly changing at the local level as states move to enact decriminalization and legalization laws. Washington and Colorado were the first states to legalize adult recreational use in 2012.1 Oregon followed suit when voters approved Measure 91 in 2014. As of July 2021, 18 states have legalized adult recreational use, 27 states have decriminalized small amounts of cannabis and 47 states have some form of state regulated cannabis program.2
Since these decisions were made almost a decade ago, public perception of cannabis has shifted. A majority (91%) of Americans think cannabis should be legal for either medical or recreational use (59%) or medical use alone (32%). The growth in public support for legal cannabis has doubled between 2000 and 2019.3 In Oregon, reported rates of current cannabis use among adults doubled from 11.6% in 2014 to 24.8% in 2021, and 62.1% of adults have ever used cannabis.4
The Overton Window + Health Impact Assessment
The Overton Window is a metaphor that describes the range of policy ideas that are politically acceptable to the general population at a given time. The concept suggests politicians can only support policies that fall within this range. Shifting the Overton Window is dependent on new ideas, social movements, and shared values in society.
Cannabis policy demonstrates a prime example of shifts in the Overton Window. Public perception of cannabis has changed dramatically over the past 20 years, enabling new policy ideas and concepts to become feasible. Contributing health evidence to this shift supports health-promoting policy.
As states legalize cannabis to various degrees, advocates and critics have formed opposing platforms that either endorse or warn of the effects of cannabis policies. Supporters say legalization frees up police resources for other matters, boosts the economy and tax revenue, and improves public health. Opponents argue that it leads to additional substance use, increases crime, and harms community health and well-being. Despite the growing body of evidence on the experience of states with legalized cannabis policies, researchers remain hesitant to make definitive conclusions on impacts because of the persistent limitations in data.5 Most existing studies are observational in design, and regulatory and funding barriers hamstring researchers in evaluating the full range of impacts of the quickly growing and diversifying supply of cannabis products and systems.6
Growing acceptance and business opportunities have catalyzed the growth and expansion of the cannabis industry. Over $10M was spent between 2019 and 2021 on cannabis lobbying in the U.S.7 One such policy approach gaining traction in the United States expands the use of cannabis by permitting consumption in public spaces.8
Due to the novelty of public consumption policies, there is limited information on which to develop an evidence-based position. This health impact assessment aims to characterize the effects of legislation that would permit public consumption of cannabis in Clackamas County and provide recommendations to mitigate negative health impacts and maximize positive ones.
The Issue: Public Consumption of Cannabis
Legalization policy has permitted cannabis use in private residences. Cannabis advocates argue that this creates inequities in access for people living in rental housing, specifically low-income renters, who do not have access to private space (such as a backyard, patio, or owned residence) where cannabis is allowed. Furthermore, the repercussions for illegal public consumption of cannabis have fallen disproportionately on communities of color through over-policing and racial profiling practices.
Policies that allow the public consumption of cannabis at public venues are seen as a possible solution to these issues, but also come with challenges. Places where public consumption is allowed, either indoors or outdoors, exposes more people to secondhand cannabis smoke, increases youth exposure to advertising, and increases the likelihood someone may drive under the influence of cannabis traveling to and from those locations.
As of September 2022, 10 states have passed laws allowing public consumption of cannabis.59 Research conducted in 2020 showed that, of the states that allowed public consumption at the time—Alaska, California, Colorado, Illinois, Massachusetts and Michigan—each had previously passed indoor clean air acts. Massachusetts was the only state among the group that did not allow public use of combustible cannabis products indoors. States attempt to mitigate the exposure to secondhand smoke by including requirements for businesses such as separation between smoking and nonsmoking areas, smoke-free areas for employees to observe on-site consumption, and controls for outdoor odor and customer visibility.9
In these states, local governments must approve the licensing of businesses allowing on-site consumption and may enact stricter laws than adopted at the state level, such as indoor smoking bans, although few localities had done so. As of June 2020, 56 localities allow on-site consumption of cannabis; however, the approach to legal requirements and local codes for business design and operation vary widely. While Massachusetts allows localities to pass laws permitting the use of public consumption of non-combustible cannabis (i.e., edibles), none had done so as of June 2020.9
| Control and Design Features | Localities |
|---|---|
| Odor control at property line | 59% |
| No smoking separation requirements | 52% |
| Ventilation or filtration system required | 38% |
| Consumption of tobacco prohibited onsite | 29% |
| Smoking only in isolated rooms | 23% |
| Restrictions placed on adult-use and/or medicinal smoking, vaping, or ingestion | 20% |
| Smoking in separate but not isolated spaces | 16% |
| Business must be in freestanding building | 14% |
| Indoor consumption only | 13% |
| Indoor smoking ban | 9% |
| Outdoor consumption only | 5% |
Table adapted from Emerging Indoor Air Laws for Onsite Cannabis Consumption Businesses in the U.S. (Thomas L. Rotering, Lauren K. Lempert, Stanton A. Glantz).
Public Consumption Policy in Oregon
Public consumption is not currently legal in Oregon. Oregon Revised Statute 475B details the time, place and manner of cannabis sales and use. Cannabis cannot be sold, smoked, vaped or used in a public place. Chapter 475B defines a public place as:
“… a place to which the general public has access and includes, but is not limited to, hallways, lobbies, and other parts of apartment houses and hotels not constituting rooms or apartments designed for actual residence, and highways, streets, schools, places of amusement, parks, playgrounds and premises used in connection with public passenger transportation.”
Legislation Introduced (2019)
In 2019, the New Revenue Coalition / Oregon NORML (National Organization for the Reform of Marijuana Laws) announced efforts to pass legislation that would legalize public consumption of cannabis in Oregon.10 HB 2233 and SB 639 were drafted to provide regulation by the Oregon Liquor and Cannabis Commission of the consumption and sale of cannabis and cannabis paraphernalia at cannabis lounges and endorsement to consume marijuana at “temporary events,” such as concerts, festivals, recreational and day-use facilities, and similar venues that require temporary venue permits. The two bills were similar, with the notable difference being that SB 639 did not authorize cannabis smoking indoors.11
The bill met significant opposition from advocates who elevated its public health impacts and direct violation of the Indoor Clean Air Act.12 There was one public hearing held on HB 2233 in the House Economic Development Committee and one held on SB 639 in the Senate Business and General Government Committee. Neither bill advanced beyond these hearings.13
HB 2233 & SB 639 (2019)
- Legalize cannabis consumption cafes to:
- Allow retailers to add all forms of tasting and consumption spaces to their businesses
- Allow stand-alone cafes where consumers can share their own cannabis products
- Create temporary event licenses that allow for regulated cannabis consumption spaces at public events
- Create opportunities for farm tourism that allows for sales and consumption to occur on licensed cannabis farms, emulating the winery model and bringing a new revenue stream for licensed farmers
- Allow for new business models such as cannabis spas and bud and breakfasts, and create opportunities for more business development and more tourism dollars to flow into Oregon
- Expand deliveries to participating hotels and temporary residences
Legislation Introduced (2021)
In 2021, the Cannabis Equity Political Action Committee introduced the Equity Investment Act (HB 3112). The bill included policies and programs designed to build wealth in communities of color, address historic harms caused by cannabis policy to those communities, and increase market diversity in the cannabis industry.14, 15
HB 3112 resurfaced provisions to allow both indoor and outdoor public consumption of cannabis at licensed sites when first introduced. Through the amendment process, the language allowing smoking and vaping of cannabis indoors was removed to comply with the Indoor Clean Air Act.
HB 3112 was profoundly different than the earlier public consumption bills by heavily focusing on equity. The bill made “equity licenses” available exclusively to groups that faced barriers to entering the cannabis industry, such as low-income residents and BIPOC community members. These same groups also had exclusive rights to obtain cannabis on-premises consumption licenses. Current and prospective business owners eligible for the equity license (low-income residents who have been convicted of a cannabis-related crime or BIPOC community members) had exclusive rights to this offering. This equity licensing program was to last until at least January 2028, at which point public consumption licenses would be made available to the cannabis business community at large. There were four public hearings before HB 3112 was referred to the Joint Committee on Ways and Means where it did not advance further.
HB 3112 (2021)
- Provision of free, automatic expungement of qualifying cannabis crimes
- Investment of cannabis tax dollars into BIPOC businesses, to programs focused on land ownership, job training, wealth creation, and reducing racial disparities in education outcomes
- Creation of an Equity Investment Governing Board to provide equity oversight for the state
- Creation of equity licenses to support BIPOC cannabis business owners that would include:
- License fee reduction and dedicated staff at OLCC to support processing times
- Provision of capital and technical support to address funding and resource inequities
- On premise consumption (smoking and vaping prohibited indoors) and expanded delivery licenses exclusive to equity licenses for a period of ten years
HIA Purpose and Background
What is a Health Impact Assessment?
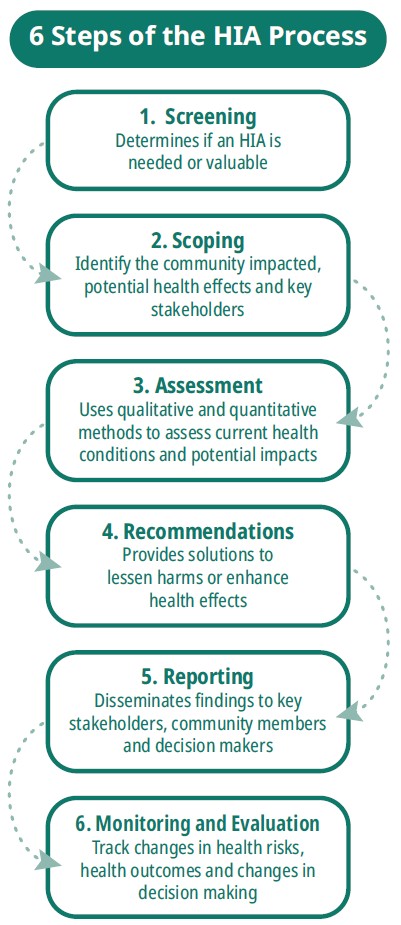
A health impact assessment (HIA) is a six-step process to evaluate the potential health benefits and harms of a decision. It can be applied to a wide range of decisions, including proposed plans, projects, programs, or policies. The systematic process (see graphic) uses a variety of data sources and methods to understand the potential effects, and distribution of those effects, on the health of a community. HIAs result in a set of recommendations to improve the outcome of a decision by considering and advancing health, safety and equity.
Purpose of this Health Impact Assessment
This HIA aims to characterize the effects of legislation that would permit public consumption of cannabis in Clackamas County and provide recommendations to both mitigate negative health impacts and maximize positive ones. The primary research question for this assessment is: What are the health, social and equity implications of public consumption of cannabis in Clackamas County? The report and recommendations from this HIA are intended to inform Clackamas County residents and decision makers, State Legislators, and the Oregon Health Authority as a public consumption policy is contemplated. It also aims to add to the knowledge base for local public health authorities across Oregon and serve as a starting point for conversations to build local capacity around this issue.
Clackamas County Public Health Division
The Clackamas County Public Health Division (CCPHD) is part of the Clackamas County Department of Health, Housing, and Human Services (H3S). Its mission is to protect and promote the community’s health by advancing racial health equity, building partnerships, and establishing culturally responsive systems. The Center for Population Health within CCPHD leads the division’s work on equity, policy, data and partnerships. Programming within the Center for Population Health include HIA consultation and the Tobacco Prevention and Education Program (TPEP).
The TPEP works to prevent and reduce tobacco use, promote smoke-free communities, reduce the influence of tobacco product marketing, and encourage tobacco users to quit. Oregon Health Authority (OHA) Health Promotion Chronic Disease Prevention (HPCDP) funds Local Public Health Authorities (LPHAs), including Clackamas County, to enforce, expand and defend the Indoor Clean Air Act. Public consumption of cannabis is an emerging public health issue that falls within this scope.
Health Impact Assessment Methods
This HIA leveraged literature review, secondary data collection, stakeholder interviews, and a framing analysis to evaluate and determine priority health areas. The scope of these investigations was to understand potential impacts at the county level. The concept of public consumption was considered in its broadest policy sense as outlined in HB 2233. This included onsite consumption at retail locations, temporary events, and production sites.
Stakeholder Interviews
24 stakeholder interviews across multiple sectors in Clackamas County gauging concerns related to public consumption policy and thoughts on mitigations. Questions were sent to interviewees in advance. Each interview lasted between 30–60 minutes.
Framing Analysis
A framing analysis to distill core perspectives and talking points of 85 public testimonies submitted on House Bills containing public consumption of cannabis policy. Testimony submitted during the hearings held for HB 2233 in 2019 and HB 3112 in 2021 were downloaded from the Oregon Legislative Information System (OLIS) website. For each session, each testimony was read once to identify major themes, and then a second time to code those themes.
For the full analysis methodology and results analysis, see Appendix II.
Literature Review + Data Collection
A framing analysis to distill core perspectives and talking points of 85 public testimonies submitted on House Bills containing public consumption of cannabis policy. Testimony submitted during the hearings held for HB 2233 in 2019 and HB 3112 in 2021 were downloaded from the Oregon Legislative Information System (OLIS) website. For each session, each testimony was read once to identify major themes, and then a second time to code those themes.
A policy scan of relevant local, state and national practices related to public consumption of cannabis and a literature review and data collection of linked health outcomes.
The literature review was conducted throughout the HIA process and direction was informed by stakeholder interviews and framing analysis results.
Health Pathway Diagram
This HIA is scoped to answer the question “What are the social, health and equity implications of public consumption of cannabis?” as well as to proactively inform decision-makers and Clackamas County stakeholders on this emerging public health issue. The health pathway diagram shows the connections between public consumption of cannabis policy and health outcomes that are evaluated in this report. Mapping how policy decisions affect health outcomes sheds light on the opportunities to influence system design to improve health. It also demonstrates how benefits and burdens are distributed among different groups, creating an opportunity to advance equity through policy design.
All changes in the outcomes included in the health pathway diagram stem from the direct increase in public places to consume cannabis that public consumption policy would create, and the continued normalization of cannabis that would be advanced.
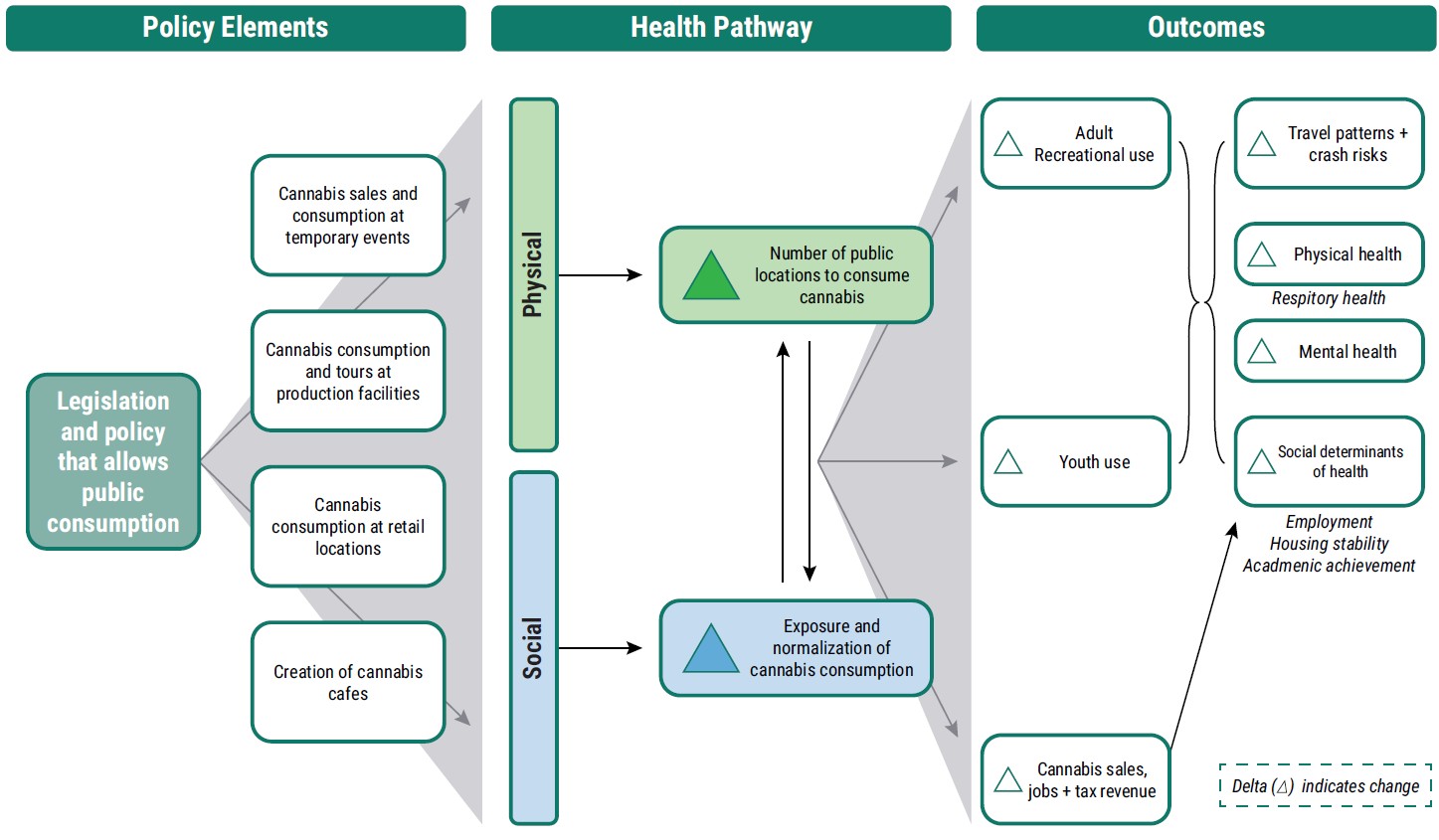
Figure 3. Health Pathway Diagram for Public Consumption of Cannabis Policy.
Key Terms and Concepts
- Equity: Equity acknowledges that not all people, or all communities, are starting from the same place due to historic and current systems of oppression, and that different levels of support (by redistributing resources, power, and opportunity) are necessary to achieve more fair outcomes. (State of Oregon Equity Framework)
- Health Equity: When all people reach their full potential and do not face barriers because of social or economic class, race, ethnicity, religion, age, disability, gender identity, sexual orientation or other social conditions. Health equity addresses poor health outcomes across an entire system by engaging the root and overlapping causes of poor health such as racism, structural disadvantage and differential privilege. (World Health Organization)
- Targeted Universalism: Targeted universalism means setting universal goals pursued by targeted processes to achieve those goals. Within a targeted universalism framework, universal goals are established for all groups concerned. The strategies developed to achieve those goals are targeted, based upon how different groups are situated within structures, culture, and across geographies to obtain the universal goal. (Haas Institute for a Fair and Inclusive Society)
- Prevention Principle: When an activity raises threats of harm to human health or the environment, precautionary measures should be taken even if some cause-and-effect relationships are not fully established scientifically. This includes: (1) taking preventive action in the face of uncertainty, (2) shifting the burden of proof to the proponents of an activity, (3) exploring a wide range of alternatives to possibly harmful actions, and (4) increasing public participation in decision-making. (Rio Declaration of 1992)
- Cannabis (vs Marijuana): The terms marijuana and cannabis are often used interchangeably but are different. Cannabis is a broad term that is used to describe the organic products that come from the Cannabis Sativa plant. This includes marijuana, as well as cannabinoids and hemp. Cannabis is the term adopted by the Oregon Public Health Division and the broader scientific community and is used broadly in this report.
Baseline Conditions
County Demographics
Clackamas County, in northwest Oregon, is one of the three counties that make up the Portland, Oregon metropolitan area. It occupies 1,870 square miles and includes 15 incorporated cities, 53 unincorporated communities and Census-designated places, and 5 hamlets and villages. Clackamas County is the third most populous county in Oregon. The 2023-estimated population is 428,168, which represents more than 13% growth since 2010.16
Most residents are between the ages of 25 and 74, and population percentages of those younger than 18 and older than 65 mirror the state of Oregon overall. The median age in the county is 42.5 years. The majority of the county is White (77.2%), followed by 2+ Races (9.48%) and Asian (5.95%), but the county has become more diverse over the last ten years. In comparison to the state, the county has a slightly larger White population (~5%) and slightly lower population of residents identifying as Some Other Race (~2.5%) but mirrors the racial demographic split otherwise.6
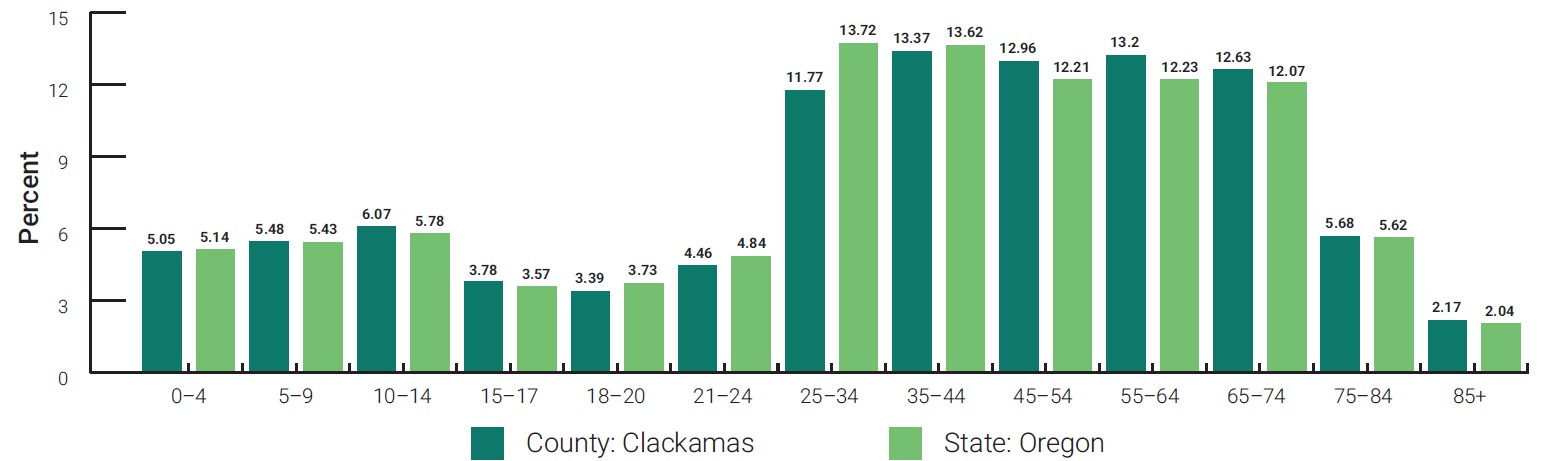
Figure 4. Population by Age. Source: Claritas, 2023.
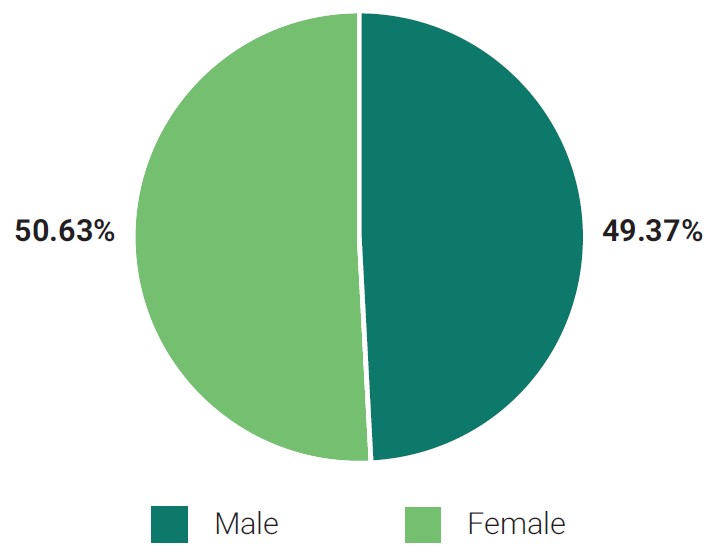
Figure 5. Clackamas County Population by Sex. Source: Claritas, 2023.
- Female: 50.63%
- Male: 49.37%
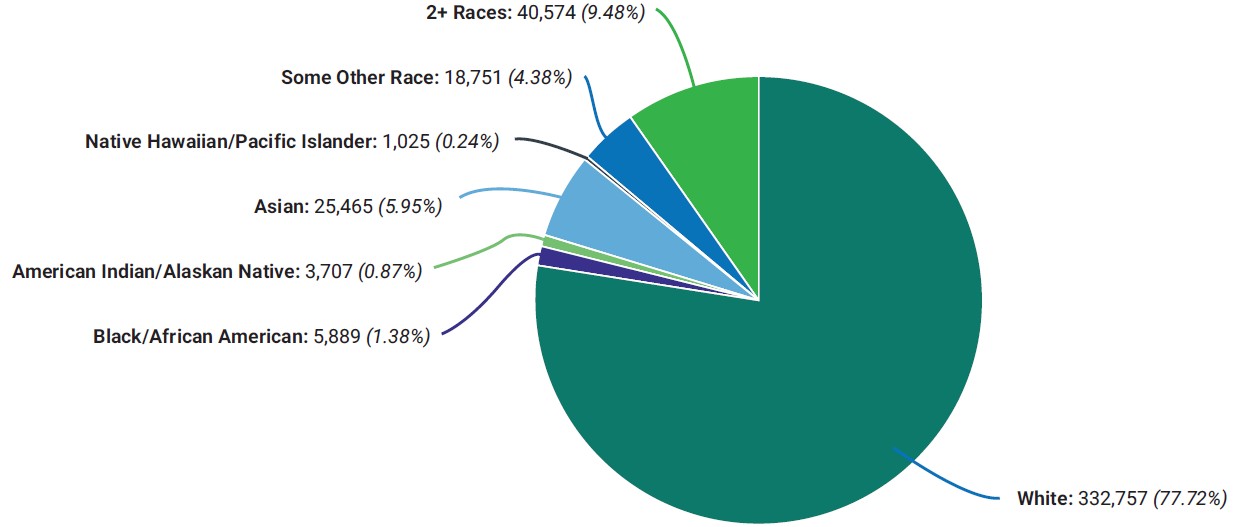
Figure 6. Clackamas County Population by Race. Source: Claritas, 2023.
- White: 332,757 (77.72%)
- 2+ Races: 40,574 (9.48%)
- Some Other Race: 18,751 (4.38%)
- Native Hawaiian/Pacific Islander: 1,025 (0.24%)
- Asian: 25,465 (5.95%)
- American Indian/Alaskan Native: 3,707 (0.87%)
- Black/African American: 5,889 (1.38%)
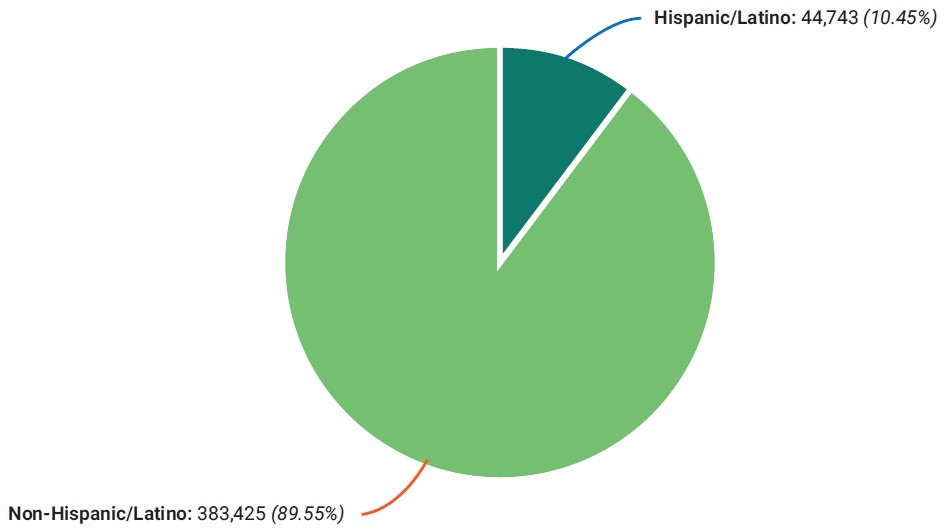
Figure 7. Clackamas County Population by Ethnicity. Source: Claritas, 2023.
- Non-Hispanic/Latino: 383,425 (89.55%)
- Hispanic/Latino: 44,743 (10.45%)
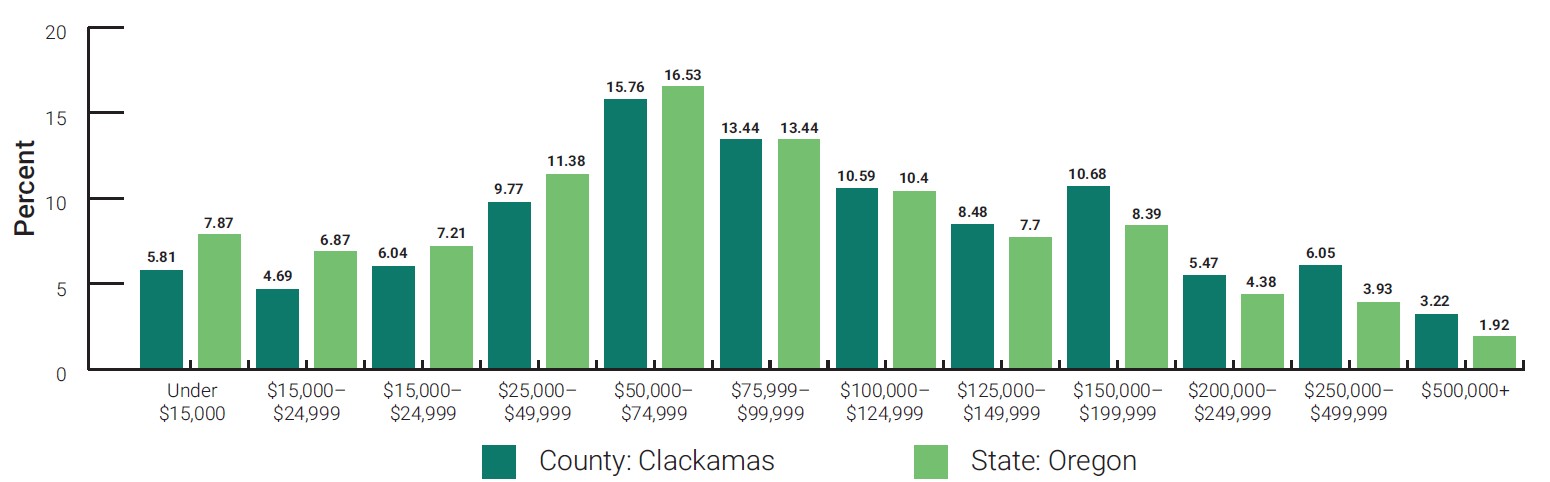
Figure 8. Population by Household Income. Source: Claritas, 2023.
Clackamas County Cannabis Use Trends
Adult Recreational Cannabis Use
In 2018, 417,000 people were estimated to have used cannabis in the state of Oregon.17 Reported current cannabis use more than doubled in the state between 2014 (11.6%) and 2021 (24.8%). Adults who report current cannabis use in Clackamas County are predominantly between the ages of 18-34, male, low-income and White. Over half of the county reports having used cannabis ever.4
Adult Medical Cannabis Use
The Oregon Medical Marijuana program reported 22,690 patients across the state in July of 2021. Most patients are adult (99.4% 18+), male (57%) and use medical cannabis to treat either severe pain (87.4%), muscle spasms (21.4%), or PTSD (15.4%). Clackamas County reported 1,524 patients (6th largest in the state), 715 caregivers (3rd largest), 489 growers (4th largest), and 430 grow sites (4th largest).61
Youth Cannabis Use
Reported rates of cannabis use within the past 30 days in 8th graders and 11th graders across Oregon trended downward between 2018-2022. This trend also held true for Clackamas County. Rates in 8th graders fell from 6.4% in 2018 to 2.2% in 2022. In 11th graders, rates fell from 20.8% in 2018 to 13.8% in 2022.64, 65, 66 In 2023, the OLCC conducted 38 Minor Marijuana Decoy operations in Clackamas County to assess retailer compliance with minimum sales age restrictions. Four locations in Milwaukie, Welches and Clackamas sold to minors.62
| Cannabis Use by: | Current^ Clackamas County (2016-2019) | Ever Clackamas County (2016-2019) | Current State of Oregon (2020) | Ever State of Oregon (2020) |
|---|---|---|---|---|
| Overall | 17.8% | 56.1% | 20.8% | 59.6% |
| Age: 18-34 | 26.5% | 66.3% | 32.6% | 64.3% |
| Age: 35-54 | 17.6% | 57.4% | 21.9% | 63.6% |
| Age: 55-64 | 15.9% | 67.1% | 16.6% | 68.2% |
| Age: 65+ | 9.1% | 33.4% | 9.7% | 44.4% |
| Gender: Female | 15.1% | 54.3% | 17.9% | 56.1% |
| Gender: Male | 21.7% | 58.6% | 23.7% | 63.2% |
| Income: <20k | 35.3% | 60.1% | 34.6% | 65% |
| Income: 20k-50k | 18.5% | 54.5% | 22.7% | 61.2% |
| Income: 50k+ | 14.9% | 59.8% | 17.9% | 62.1% |
| Ethnicity: Latinx | 13.5% | 53.8% | 18.4% | 49.1% |
| Ethnicity: Non-Latinx | 18.3% | 56.6% | 20.9% | 60.8% |
| Cigarette Smoker: Current Smoker | n/a | n/a | 44.1% | 86.5% |
| Cigarette Smoker: Not a Smoker | n/a | n/a | 17.4% | 55.5% |
| Source: Oregon Health Authority, 2022. ^Current cannabis use means use at least once in the past 30 days. | ||||
Existing Cannabis Regulatory Systems
Oregon Cannabis Regulation
The Medical Marijuana Act passed in Oregon in 1998 through Ballot Measure 67. The measure permitted the cultivation, possession, and use of cannabis by doctor recommendations for select medical conditions (including chronic pain, glaucoma, PTSD, muscle spasms, and seizures).19 The measure passed with 54.6% support.
Recreational marijuana became legal for personal use in Oregon on July 1st, 2015, following the passing of Measure 91, the Control, Regulation, and Taxation of Marijuana and Industrial Hemp Act, in November of 2014. General market sales of cannabis through existing medical dispensaries began in October 2015, and full market sales began in November 2016.
The passage of Measure 110 in 2020 altered how marijuana tax dollars are distributed, specifying that $11.25M per quarter is reserved for the State School Fund (40%); Mental Health, Alcoholism, and Drug Services (20%); Oregon State Police (15%); Oregon Health Authority for Drug Treatment and Prevention (5%); and Cities and Counties (20%). Amounts exceeding $11.25M in a quarter are distributed to the Drug Treatment and Recovery Services Fund.20 Although retail sales rose dramatically during the pandemic, they have since receded. The Oregon Office of Economic Analysis attributes this decline to an oversupply of product and a saturated retail market that have driven down prices for consumers.21
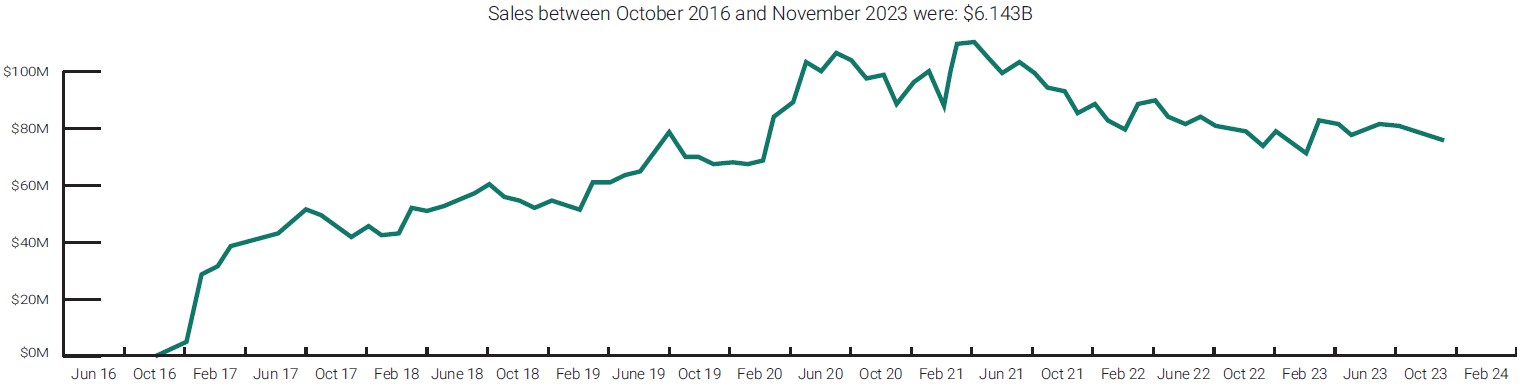
Figure 9. Marijuana Retail Sales in Oregon, October 2016-November 2023.
Marijuana sales in Oregon rose steadily in the years leading up to the pandemic; in March 2020, they rose drastically. They have since fallen, with sales dipping below the pre-pandemic peak in August 2019 six times between November 2022-November 2023.
Source: Oregon Liquor and Cannabis Commission.
Several state departments and advisory boards make up the cannabis governance framework in Oregon. The Oregon Department of Agriculture (ODA) oversees production and processing licensing, inspections, and oversight. The Oregon Liquor and Cannabis Commission (OLCC) oversees regulation of wholesale, retail, and distribution licensing for cannabis products (including CBD products and medical grade products) sold through licensed retail shops. OHA regulates products sold at medical cannabis dispensaries and oversees the Public Health Medical Marijuana Program.
The Oregon Cannabis Commission (OCC) was established in 2017 and provides advice to both OHA and the OLCC on cannabis regulation, advances strategic plans to maintain affordable medical cannabis access, and monitors trends in cannabis regulation and policy. In the 2019 OCC Report, the commission recommended that the state create the Cannabis Research Center (CRC) to expand the science and research related to the health effects of cannabis.22
A Note on the COVID-19 Pandemic
Several cannabis regulatory changes occurred in response to the COVID-19 pandemic that began in Oregon in March of 2020, and were later made permanent in September of 2020:
- Allow for curbside pickup, including through exterior windows
- Allow for retail delivery
- Allow for online sales and purchasing
- Deferred and waived fees
- Acceptance of expired IDs
These changes sought to minimize the transmission of the virus in retail settings, reduce economic harms to cannabis businesses, and balance hardships experienced by medical cannabis users. These changes were made to acknowledge the evolving contexts and risks the general population was experiencing that may affect their cannabis use, like increased use related to stress, increased availability of cannabis products in the home, and disproportionate impacts these changes have on communities experiencing compounding inequities.60
Clackamas County Cannabis Regulations
Clackamas County zoning law permits cannabis retailers to operate in most commercial zones, both urban and rural. Several minimum separation requirements exist, including:
- 2000 feet from a public elementary or secondary school
- 1500 feet from a public park, public playground, government-owned recreational use, public library, substance use disorder service provider licensed by OHA, light rail transit station, or a multifamily dwelling owned by a public housing authority
- 500 feet from a licensed daycare facility or licensed preschool23
As of March 2019, Clackamas County passed Zoning Ordinance 271, which authorizes just one recreational cannabis grow site on a tract of land in Ag/Forest (AG/F), Exclusive Farm Use (EFU) or Timber (TBR) zoning districts. A vast majority of the county is zoned to permit production facilities, however this zoning law only applies to unincorporated Clackamas County. Individual cities may designate different zoning districts permitted for cannabis retail or production. Five cities in Clackamas County have prohibited the establishment of licensed recreational cannabis producers and retail in Clackamas County: Lake Oswego, Sandy, West Linn, Canby, and Wilsonville.24
As of December of 2022, there were 824 active cannabis retailers in the state of Oregon, and 35 cannabis retailers in Clackamas County.26 Of these, only five operated outside of the Metro boundary in Clackamas County: Molalla (2), Aurora (1), Rhododendron (1) and Welches (1).
The largest number of cannabis related permits in Clackamas County are for production facilities, with 195 registered production facilities in December of 2022.63 This figure reflects facilities that produce recreational cannabis and are registered through the OLCC. Cannabis production and growing is permitted in urban industrial, exclusive farm use, ag/forest, timber, rural residential farm-forest 5-acre, farm-forest 10-acre and rural industrial zones.
In comparison to other counties, Clackamas has a large number of recreational producer licenses, and a vast majority of the county is zoned to allow recreation production (planting, cultivation, and harvesting of cannabis).
- 195 Recreational Producers
manufacturing, planting, cultivation, growing or harvesting of cannabis - 43 Recreational Processors
processing, compounding or conversion of cannabis into cannabinoid products, excluding packaging or labeling - 22 Recreational Wholesalers
purchasing cannabis items in Oregon for resale to a person other than a consumer in Oregon - 35 Recreational Retailers
selling cannabis items to a consumer in Oregon
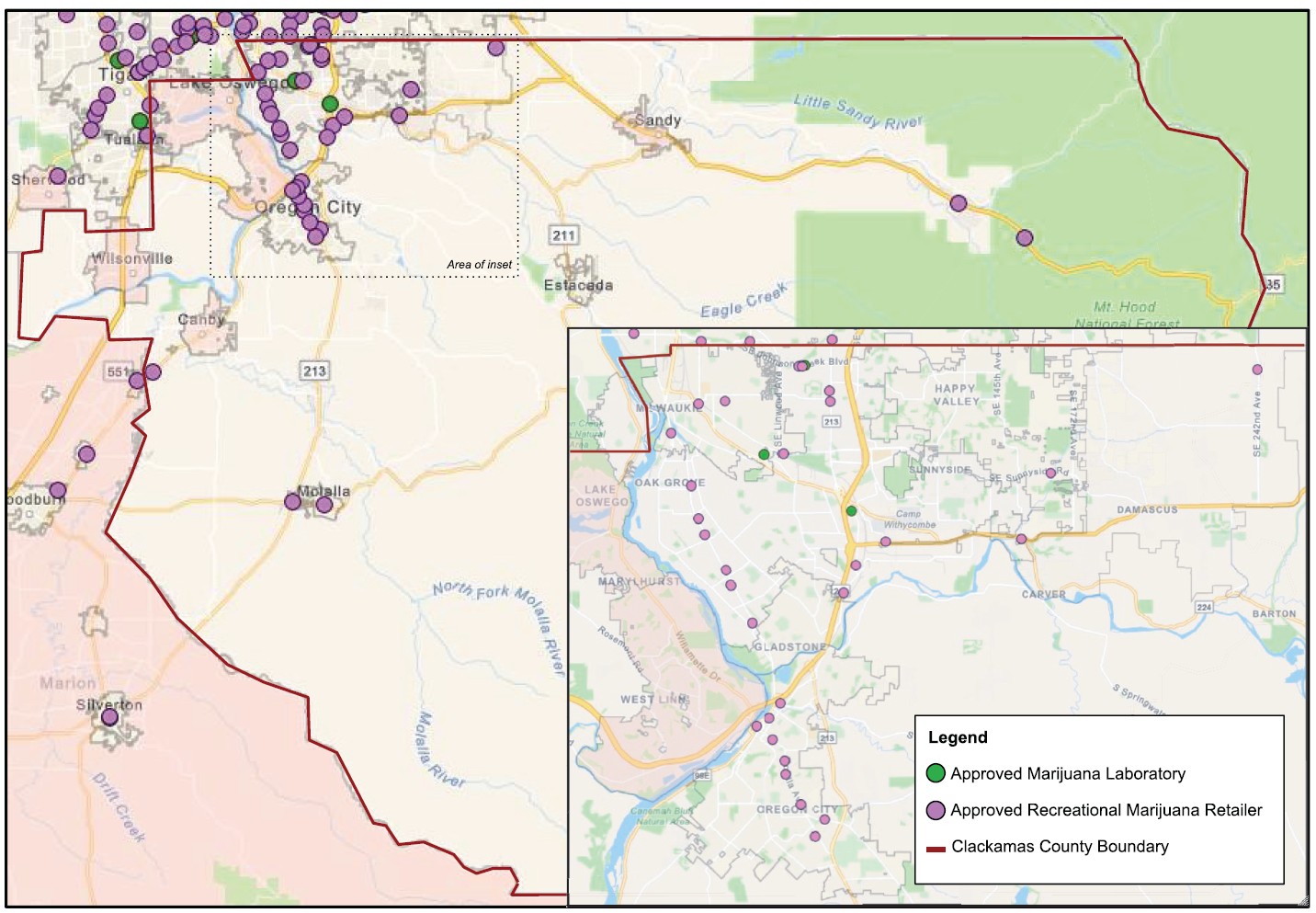
Figure 10. Approved Marijuana Retail and Lab Locations.
Clackamas County marijuana retailer and laboratory locations as of December of 2022. The cities of Lake Oswego, West Linn, Wilsonville, Canby and Sandy do not allow marijuana retailers to operate. INSET: Each of the three laboratories in the county and most retailers are located within the Metro boundary extending into the northwest corner of the county. Adapted from the Oregon Liquor Control’s Map of Oregon Recreational Marijuana Retailers and Labs map.
Assessment
The assessment draws on data and scientific literature, interviews with 24 stakeholders, and testimonies submitted in favor and opposition of previous legislation to recommend actions that could mitigate harm and maximize benefit if public consumption of cannabis is legalized in Oregon.
Social Normalization of Cannabis
Normalization means becoming a ‘normal part’ of leisure and lifestyle and no longer considered potentially harmful. The decriminalization of cannabis in an increasing number of states and the development of medical and recreational cannabis laws has contributed towards its normalization. State cannabis markets are expanding production to meet growing demand, making cannabis available in a variety of products.27 Four methods of consumption are most common: inhalation (smoking or vaping), ingestion (edibles or beverages), sublingual absorption (oils or lozenges), or skin application (lotions or salves). This variation in product availability expands the audiences who may be interested in cannabis use. Trends in cannabis mode use have fluctuated in recent years and are difficult to monitor. Surveillance shows inhalation is still the dominant form of consumption, but multi-modal consumption is rising, and use varies within age groups.28, 29, 18 Use of more potent cannabis products like vaping oils and cannabis extracts is increasing in prevalence in 16–19-year-olds in the U.S.30
As social acceptance of cannabis use has increased, it is perceived as less harmful than other substances like tobacco or alcohol. Normalization of cannabis is evident, as discussion has shifted from a substance once considered harmful and privately used, to one that has a degree of acceptability in different spaces (i.e., concerts). The number of adults that report seeing marijuana advertisements in their community across Oregon increased by 51% between 2015 and 2018, with 2/3 of adults reporting seeing marketing. However, many adults in Oregon (60%) think marijuana marketing should not be in areas seen by people under 21, and 43% of people think there is too much marijuana marketing in their community.16
The public health field has spent considerable time and resources to combat the normalization of tobacco smoking in public places. A primary concern associated with public consumption of cannabis is the risk of renormalizing all forms of smoking (including regular combustible cigarettes and e-cigarettes) to all ages, including youth.8 Legalization of marijuana has been shown to decrease the perceived harm of cannabis among youth. A study evaluating perceived harm on 8th and 10th grade students in Washington and Colorado found that there was a decrease in perceived harm of marijuana and slight increase in use.31
Cannabis and Physical Health
Cannabis and cannabinoids have a wide range of applications that demonstrate some therapeutic effects. Modest evidence exists showing the benefits cannabis consumption has on treating the side effects of chemotherapy, managing chronic pain, improving sleep, and spasticity symptoms associated with multiple sclerosis. There is limited evidence showing the benefits of cannabis consumption in increasing appetite for HIV/AIDS patients, improving symptoms of Tourette Syndrome, improving outcomes after traumatic brain injuries, and treating anxiety and PTSD.36
Research on cannabis use and cancer incidence is limited. There is moderate evidence showing that there is no association with cannabis use and lung, head or neck cancers. Largely, for most other cancers there is insufficient evidence to support or refute a connection to cannabis. Studies have linked long-term cannabis smoking with poor respiratory outcomes and frequent chronic bronchitis. There has not been robust evaluation to understand the associations between cannabis and all-cause mortality, occupational injuries, or cannabis overdose. However, moderate evidence exists showing that in states that have legalized cannabis, increases in pediatric overdose and respiratory distress follows.36
Cannabis and Secondhand Smoke Exposure
The Indoor Clean Air Act (ICAA) was passed in 2001 to protect employees and the public from exposure to secondhand tobacco smoke, a known cause of cancer. In 2007, the law expanded and removed preemption, giving local jurisdictions the ability to tailor the ICAA to their community. The expansion exempted cigar bars and created smoke shops. Inhalant delivery systems (e-cigarettes) and cannabinoids were added to ICAA in 2015.
Indoor particulate matter, regardless of source, can penetrate deep in the lungs. This can cause nose and throat irritation, as well as aggravation of existing heart and lung conditions.32 Physiologically, PM2.5 exposure has been shown to cause inflammatory reaction and oxidative stress in cells, which are the mechanisms leading to negative health outcomes.33
As with tobacco, secondhand smoke from cannabis is a primary concern. When smoked indoors, cannabis smoke has been shown to have a PM2.5 emission rate that is 3.5x higher than tobacco smoke.35 An evaluation of a cannabis dispensary in California that permitted on-site consumption found that PM2.5 concentrations were 28x higher during operation hours than when the business was closed. Concentrations ranged from 50 to 200 μg/m3, which far exceeds the 10 μg/m3 threshold where decreased endothelial function occurs and can cause health problems for some individuals.36
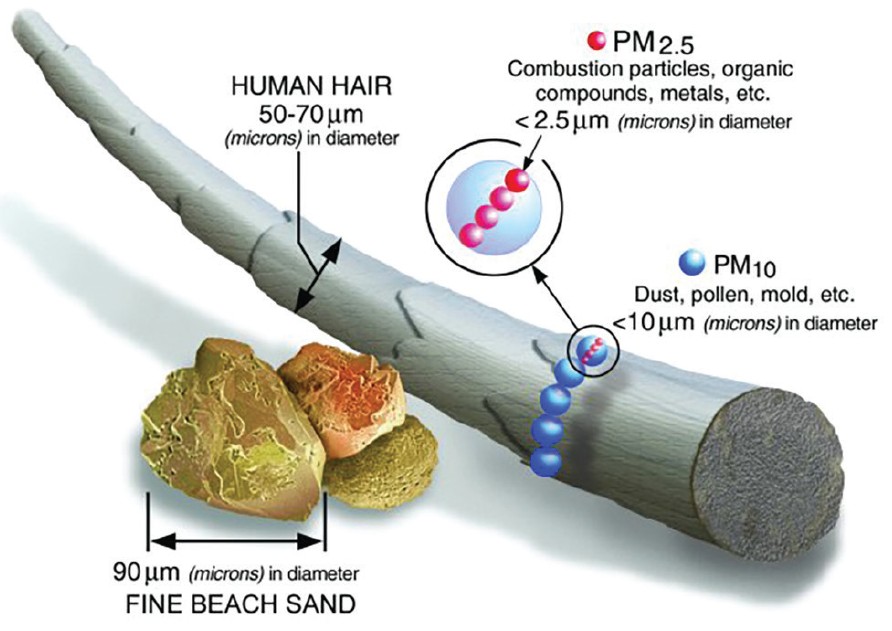
Figure 11. PM2.5 Size Comparison.
Particulate matter, abbreviated as PM, is the term for a mixture of solid particles and liquid droplets found in the air. PM is measured in microns, represented by the figure μg. Fine inhalable PM includes those particles with a diameter of 2.5 μg or smaller and written as PM2.5. Smoke from combustible materials, such as firewood or a lit cigarette or cannabis joint, produces PM2.5.34
Source: Environmental Protection Agency
Although indoor design features intended to alleviate smoke, like ventilation and odor control systems, are required of businesses licensed by some localities, these measures have proven to be inadequate to safely protect employees and patrons against the health effects of secondhand smoke exposure.9 In the case of the California cannabis dispensary assessment, measurements indicated that the installation of a ventilation system reduced the average PM2.5 by only 12.2%, which was not statistically significant.36 The American Society of Heating, Refrigeration, and Air Conditioning Engineers (ASHRAE) commented on these types of solutions, “…the only means of avoiding health effects and eliminating indoor [Environmental Tobacco Smoke] exposure is to ban all smoking activity inside and near buildings.”37
Cannabis and Road Safety
Many factors impair a driver’s performance. Examples include alcohol, drugs, fatigue, distraction or emotional states. All of these can decrease a driver’s ability to perform driving tasks to a “normal” safe degree. Cannabis is absorbed differently in the body than alcohol, and decays at a faster rate. This makes it difficult to study, monitor, and enforce because there is limited knowledge on how cannabis affects driving ability, and legal limits that work for alcohol do not apply.
Early evidence from states where cannabis is legal shows an increase in cannabis-related crashes.38 Studies indicate that driving under the influence of cannabis increases the risk that a driver will be in a fatal crash, and even more so when consumed with alcohol.39 To provide guidance to protect road safety as the research develops, states have adopted a variety of laws regulating cannabis and driving. As of 2018, at least 12 states had adopted zero tolerance laws and 6 states adopted laws that established threshold concentrations that it is illegal to drive within. While it is illegal to drive under the influence of cannabis in Oregon, as of 2022 there is no zero-tolerance law or established threshold concentration.40. 41
Between 2012 and 2016, OHA reported 81 fatal crashes in Oregon that were related to marijuana use. Many of these crashes (62%) also involved another substance, namely alcohol.42
| Health Outcome | Clackamas County | State of Oregon | Sources |
|---|---|---|---|
| Age-Adjusted Death Rate Due to Motor Vehicle Traffic Collisions | 9.6 per 100k | 11 per 100k | CDC, 2017-2019 |
| Alcohol-Impaired Driving Deaths | 39.3% | 31.5% | County Health Rankings, 2015-2019 |
Cannabis and Mental Health
Studies have found a strong association between frequent cannabis use and the development of schizophrenia and other psychoses. There is moderate evidence linking regular cannabis use with increased mania in patients with bipolar disorders, as well as increasing social anxiety. There is also moderate evidence linking heavy cannabis use with increased suicidal ideation, attempt, and completion.6
| Health Outcome | Clackamas County | State of Oregon |
|---|---|---|
| Death Rate to Suicide | 12.5 per 100k | 20.8 per 100k |
| 8th graders who have attempted suicide | 4.5% | 5% |
| 8th graders who have considered suicide | 12.4% | 11.6% |
| 11th graders who have attempted suicide | 6.2% | 6.8% |
| 11th graders who have considered suicide | 19.1% | 16.9% |
Sources: Oregon Health Authority, 2019; Oregon Health Teens Survey, 2019
Cannabis and the Social Determinants of Health
The social, physical and environmental conditions we live in impact our health and wellbeing more than the medical care we receive. The interactions between health, social, and environmental factors is complex. Limited evidence exists on the way cannabis use influences the social determinants of health outlined below, and it is important to consider possible impacts in light of other contributing factors.
Academic Achievement
While cannabis use has been associated with acute impairment of memory and attention, there is limited evidence that links cannabis, academic achievement, and education outcomes.6 While some studies have linked cannabis use with high school dropout status, updated research highlights how cannabis use and drop out status have several shared underlying causes, such as deviant behavior and family dysfunction.43%
Employment
There is no consensus on how cannabis impairment is defined, making it difficult to discern the total impact of cannabis in the workplace. While increases in workplace incidents have been identified in employees in industrial sectors who test positive for cannabis use, the current body of evidence does not support an overall position on cannabis use and risk of occupational injury.44, 45
There is limited evidence that shows a connection between cannabis use and unemployment.6 Researchers found that there was no impact on employment, hours, or wages for adult workers in states with medical cannabis laws.46 A recent study focused on Colorado counties found a 4.5% increase in overall number of employees and .7% decrease in unemployment to be associated with the sale of recreational cannabis in dispensaries.47
Housing
Renters who have a medical or therapeutic need to use cannabis may find it difficult to obtain housing. In some cases, continued use by them or members of their household could put their housing stability at risk.
Many landlords and rental property owners establish smoke-free policies that prohibit the use of combustible substances like cannabis. In Oregon, these policies are applicable to recreational and medical cannabis users alike as patients of the Oregon Medical Marijuana Program with a disability, for example, are not protected under the Americans with Disabilities Act (ADA) or any state anti-discrimination laws.48
Stricter policies are found at the federal level and apply to public housing properties across the country overseen by the U.S. Department of Housing and Urban Development (HUD). Households otherwise qualifying for residence in these properties would have their admission denied if their members are identified as cannabis users. Likewise, current households residing as tenants may be subject to eviction if cannabis use is determined.49
| Social Determinant of Health | Clackamas County | State of Oregon | Sources |
|---|---|---|---|
| High School Drop Out Rate | 2.0% | 2.4% | OR Dept of Ed, 2019-2020 |
| 8th Grade Students Proficient in Math | 44.1% | 37.3% | Annie E. Casey Foundation, 2018-2019 |
| 8th Grade Students Proficient in Reading | 58.0% | 53.2% | Annie E. Casey Foundation, 2018-2019 |
| Cannabis Use – Employed or Self Employed | 16.7% | 20.8% | OHA, 2016-19; OHA, 2020 |
| Cannabis Use - Unemployed | 35.3% | 39.5% | OHA, 2016-19; OHA, 2020 |
| Number of Rental Units^ | 47,230 | 636,811 | ACS 5-Year Estimates 2021 |
| Number of Public Housing Units^^ | 444 | 2,800 | HUD, 2021 |
^Determined by adding Renter Occupied Housing Units; Vacant – For Rent; and Vacant – Not Rented, Occupied data.
^^Only includes units managed by local housing agencies. Does not include units where vouchers are used to obtain housing.
County Stakeholder Interviews
The stakeholders interviewed for this HIA represent a wide range of sectors. This created divergent and at times conflicting perspectives on the impacts of public consumption of cannabis policy. Interviews took place in the winter of 2019, prior to the introduction of HB 3112; as such, participants were only asked about HB 2233.
The top concern for county stakeholders regarding current cannabis consumption use is the associated impact on mental health outcomes.
Current Impacts of Cannabis Use
When asked what are the current impacts stakeholders are seeing with recreational cannabis (with no public consumption policy enacted), the top responses were ‘Worsens Mental Health’ and ‘No Impact’ (Figure 11). Concerns around mental health included disproportionate impacts on youth and how cannabis can lead to or can exacerbate conditions like depression, anxiety, suicidality, and psychosis. When discussing the current impact of cannabis, stakeholders described how it was a non-issue in their field of work, mainly administrative roles for public services or in the cannabis retail field.
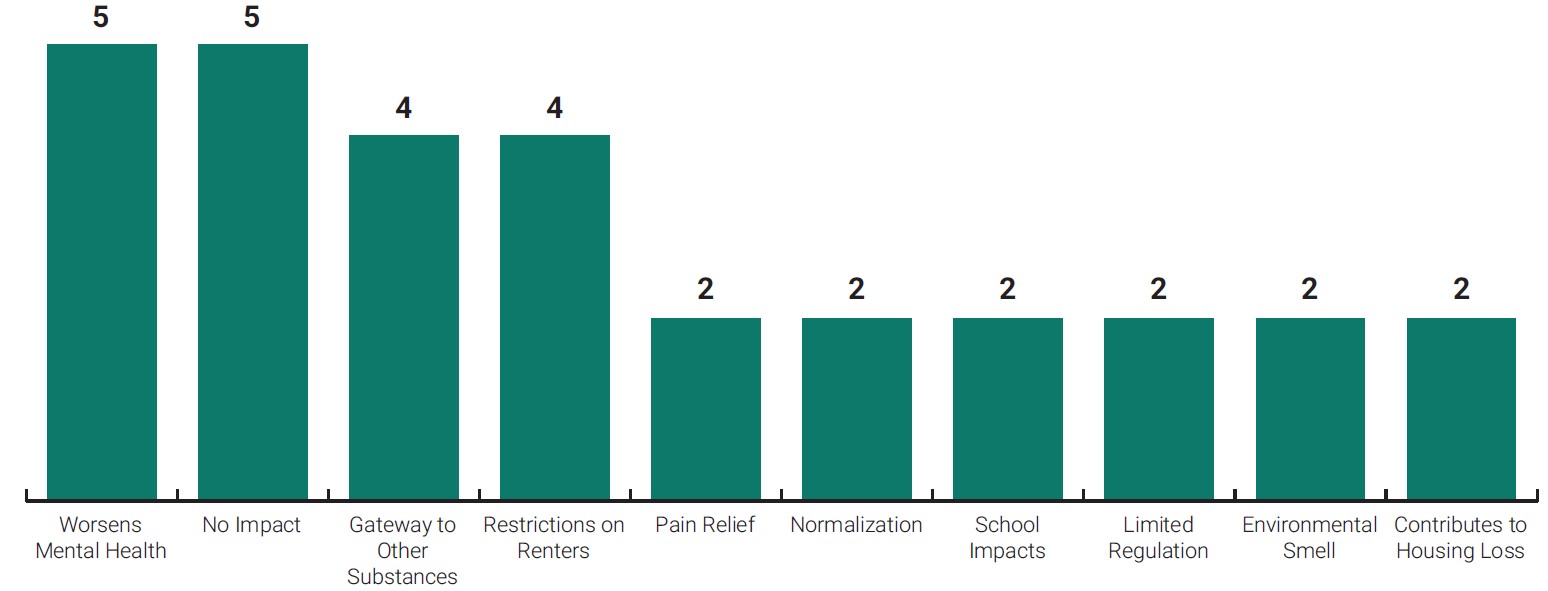
Figure 12. Top Existing Impacts from Cannabis (Without Public Consumption Policy).
Anticipated Impacts of Public Consumption of Cannabis Policy
The impact of most concern associated with state-enacted public consumption of cannabis is increased normalization and use.
When asked what are the anticipated impacts of public consumption policy in the county, the most cited were increased normalization and use. Stakeholders suggested that legalizing public consumption of cannabis would lead to greater access and acceptance of cannabis by the public, which was viewed both positively and negatively by participants. Some stakeholders thought that public consumption would lead to revenue and public support (positive) or more use of other substances and mental health impacts (negative).
Primary negative impacts of concern for stakeholders were decreases in road safety from driving under the influence of cannabis, widening the pathway to other substances by increasing access to cannabis, exacerbating respiratory health outcomes for cannabis smokers and people experiencing secondhand smoke, and complaints related to increased community cannabis use. Primary positive impacts cited by stakeholders included supporting local cannabis business revenue, employees, and associated economic markets, and increasing access to cannabis to people who have no space to consume.
Distribution of Benefits and Burdens from Public Consumption of Cannabis Policy
When asked who would benefit from public consumption of cannabis policy, the most frequently mentioned benefactors were local cannabis businesses. Public consumption policy would drive demand, increase sales opportunities, and create more career paths. The next most frequently cited were people consuming medically prescribed cannabis in additional locations and the programmatic recipients of cannabis-related tax dollars like schools and enforcement programs.
Groups that BENEFIT from public consumption policy
(ordered by frequency)
- Local cannabis businesses
- Medical cannabis patients
- Cannabis tax recipients
- Tourism industry
- Small businesses
- Recreational users
- Renters with restrictions
- Cannabis industry
Groups that are HARMED by public consumption policy
(ordered by frequency)
- General public
- Youth
- People driving
- Low income households
- People in recovery
- Public safety officers
- Grow site neighbors
- People with mental health diagnoses
When asked who would be harmed, the most common response was the general public at large. This was largely attributed to being exposed to secondhand smoke from cannabis consumption. The second most frequently cited group was youth. Youth were cited for two primary reasons: 1) the impacts of cannabis on developing brains, and 2) the social costs of cannabis consumption like missing school and consuming other substances. Relatively few stakeholders (2) mentioned that the policy may have potential impacts specific to communities of color because of historical inequities and discrimination in cannabis policy.
When asked what solutions would address challenges created by public consumption of cannabis policy, the most suggested ideas were place-based health and safety regulations, bolstering enforcement resources, clarifying consumption regulation structures, developing education systems for bud tenders, and conducting ongoing research and surveillance on impacts.
For the results from the stakeholder interviews in full detail, see Appendix I.
Legislative Testimony Framing Analysis
Frames are conceptual models about the way the world works. They help us make sense of new information we receive and serve as filters through which we categorize information and derive meaning from them, either consciously or unconsciously. Understanding how issues are framed is important for advocates to anticipate how policies will be received by decision-makers. Effective framing to advance health equity links decision-makers’ values with structural and environmental changes that promote health and reduce disparities.50
HB 2233 Summary
HB 2233 would have empowered the Oregon Liquor and Cannabis Commission (OLCC) to regulate the consumption and sale of marijuana items at temporary events, including the licensure of premises hosting events. The OLCC would have also regulated consumption at and licensure of cannabis lounges, including requiring them to obtain a sanitation certification from OHA. Local options for cities and counties would have also been created by the bill.
HB 2233 Analysis
Five sectors representing the local cannabis industry, public at large (residents), government actors, advocacy groups in general, and advocacy groups focused on health issues submitted 28 testimonies. The two most prominent sectors were the local cannabis industry and the public at large (residents). A narrow majority of testimonies submitted were in support of HB 2233. The most common frames in support of the bill were Cannabis Equity - Use and Support Business. The most common frames used in opposition to the bill were Indoor Clean Air Act (ICAA) & Health and Impacts Youth.
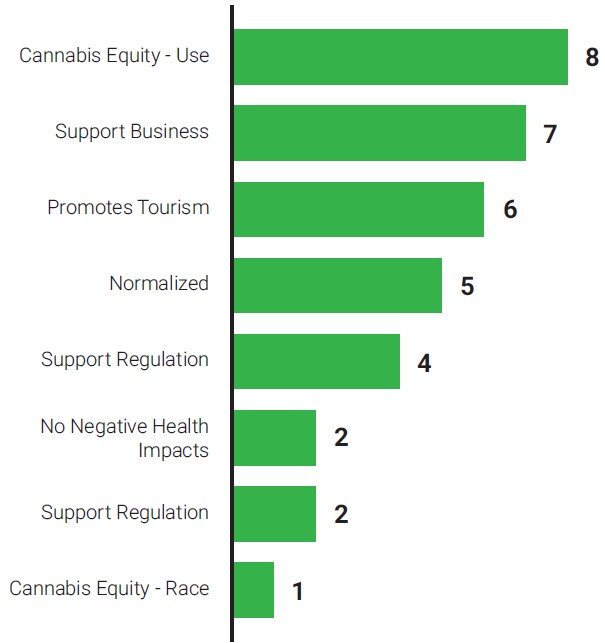
Figure 13. Frame Counts in Support of HB 2233.
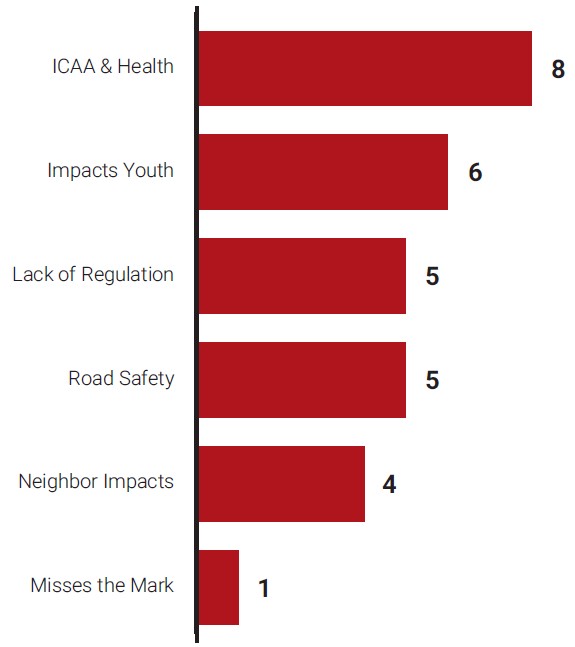
Figure 14. Frame Counts in Opposition of HB 2233.
| Stance | Frame | Frame Description | Example Quote |
|---|---|---|---|
| Support | Cannabis Equity - Use | Communities need safe places to use cannabis, especially those in public housing. The current system creates inequity. | “…there are many people in our communities who live in public housing or rentals where cannabis possession and use is disallowed. Meanwhile, those of us who own homes are free to possess and consume cannabis freely. This creates an economic inequity, where people who can afford to purchase a home are able to benefit from legal cannabis, while poorer individuals are essentially prohibited from using a legal product.” “Right now we are leaving our patients out in the cold, literally, by forcing them to break the law and stand on the street in order to get the quick relief of inhaled cannabis (such as nausea due to chemotherapy) |
| Support | Supports Business | Cannabis consumption will support local businesses and business owners, trickle over into other industries, and fuel Oregon's economy. | “HB 2233 solves a critical problem in that cannabis consumers and producers from around the state are hampered by a cannabis legalization policy that is half finished; cannabis is legal yet there is virtually nowhere to consume it.” |
| Oppose | ICAA & Health | Public consumption of cannabis would lead to violation of the Oregon Indoor Clean Air Act, exposing workplace employees and Oregonians at large to harmful secondhand smoke. | “HB 2233 solves a critical problem in that cannabis consumers and producers from around the state are hampered by a cannabis legalization policy that is half finished; cannabis is legal yet there is virtually nowhere to consume it.” |
| Oppose | Impacts Youth | Increasing exposure of cannabis consumption will harm youth and increase the risk of use. | “I am new to this state and utterly amazed at how common and normal it is for youth to engage in smoking….Allowing for public consumption, cafes and licenses at special events, we would be further allowing our children to believe that marijuana is safe and ok to use.” |
HB 3112 Summary
Coined as the “cannabis equity bill,” HB 3112 would have:
- Established a Cannabis Equity Board within the Office of the Governor to provide equity oversight of the state’s cannabis industry. Annual findings and reports to an interim committee of the Legislative Assembly would be required. Established equity liaisons at Oregon Health Authority and Oregon Liquor and Cannabis Commission to report to the Cannabis Equity Board quarterly on specified information.
- Established a Cannabis Equity Fund and continuously appropriate moneys in the fund to the Cannabis Equity Board for specified purposes.
- Directed the Oregon Liquor and Cannabis Commission to issue equity licenses to qualified applicants and issue cannabis on-premises consumption licenses, cannabis delivery licenses, and shared processing licenses or shared processing facility licenses to applicants who meet qualification criteria for the equity license. After January 1, 2032, the Commission could issue cannabis on-premises consumption licenses, cannabis delivery licenses, and shared processing licenses or shared processing facility licenses to applicants who do not meet qualification criteria for the equity license.
- Created a process and modified procedures at the Office of Public Defense Services, Judicial Department, and Oregon State Police to set aside convictions, arrests or charges for marijuana offenses. Entities maintaining records of parole, probation or post-prison supervision violations would be required to review and expunge any records of violations.
HB 3112 Analysis
Fifty-eight documents submitted as testimony were reviewed. Seven different sectors were identified: Local cannabis industry representatives, law firms, the public at large (residents), government actors, academic institutions, advocacy groups focused on health issues, and advocacy groups focused on culturally specific services and communities of color. The most common frame used in support of the bill was Racially Just Policy and was cited in 92% of testimonies in support of the bill. The most common frame used in opposition was Color Blind Policy.
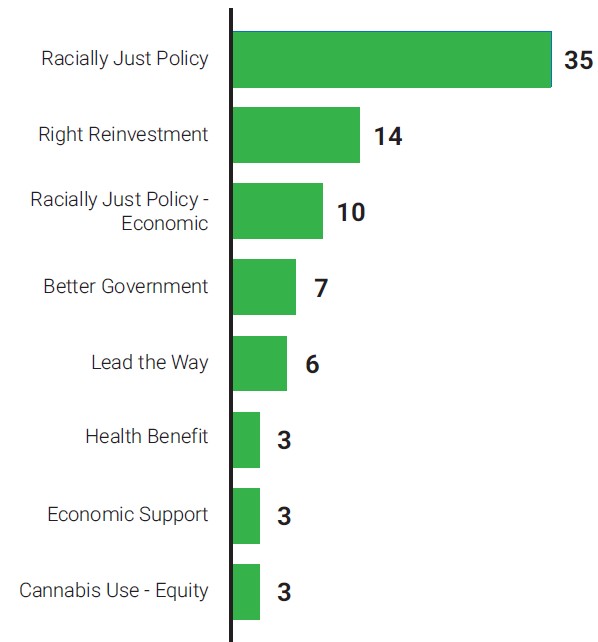
Figure 15. Frame Counts in Support of HB 3112.
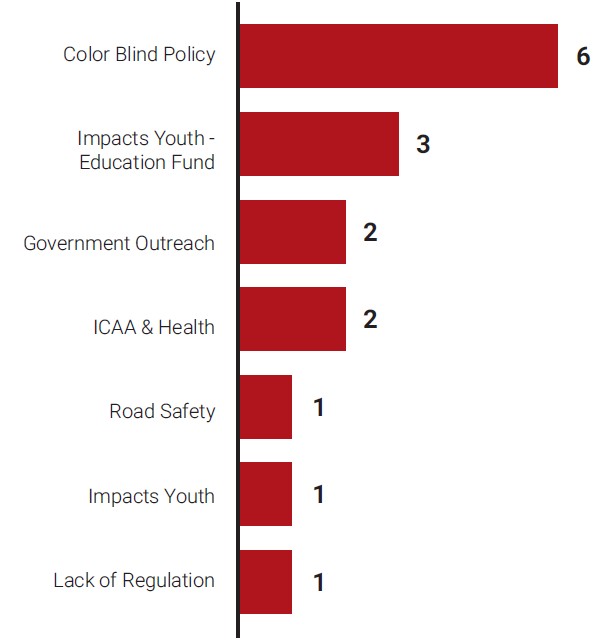
Figure 16. Frame Counts in Opposition of HB 3112.
| Stance | Frame | Frame Description | Example Quote |
|---|---|---|---|
| Support | Racially Just Policy | HB 3112 will enact policies that will center and benefit communities of color who were disproportionally impacted by cannabis regulation, prohibition, and criminalization in the past during the War on Drugs. | “This bill is a form of reparations that BIPOC communities are due after centuries of racism and white supremacy dominating this county.” “We recognize that over 100 years of draconian cannabis policies and disparate cannabis related arrests, convictions, and sentencing have had long-lasting legal, social, economic, and inter-generational consequences to these specific communities.” |
| Support | Right Reinvestment | Reinvestment of cannabis tax revenue back into communities of color that have experienced the most harm from the industry is a just investment and good use of public dollars. | “We, as consumers, cannabis business community, and simply concerned citizens, believe the use of cannabis tax revenue to repair harm done to Black, Indigenous and Latinx communities is an appropriate and necessary way to restore rights and opportunities.”. |
| Oppose | Color Blind Policy | HB3112 is not fair because it only benefits a small group of people, determined by race. | “When the word “equity” is used, it is about creating new power structures that benefit the chosen few. The inclusion of "equity" in almost every bill is starting to divide the state. It is the furthest thing from unity as you could get. Redistribution of fairness is not equity.” |
| Oppose | Impacts Youth – Education Fund | Increasing exposure of cannabis consumption will harm youth and increase the risk of use. | “Taking away 40% of the Oregon Marijuana Account from funding the State School Fund with no way to make up for it. You cannot take more away from our children. This is heartbreaking to deny this to the ones that need this money the most.” |
HB 2233 and HB 3112 Comparison
During both sessions, most of the testimonies were submitted in support of the bills. However, because the policy levers within each bill were significantly different, the framing and testimonies were as well. Key differences are described below.
- Stakeholders. During the session for HB 2233, testimonies came from cannabis businesses, citizens, government agencies, and community based and health advocacy groups. During the session for HB 3112, testimonies came from lawyers and academic institutions, as well as the same stakeholders for HB 2233. Fewer health advocacy groups testified in HB 3112. This may have been a product of the COVID-19 pandemic, which limited participation from the health field.
- Conversation. Testimonies in support of HB 3112 reflected the leading issues in the bill that centered racial equity and justice verses HB 2233 that focused on the consumption of cannabis at public events and venues. Frames around equity almost entirely shifted to center communities of color in HB 3112 as opposed to low-income renters in HB 2233.
- Opposition Shift. Despite the increase in testimonies between sessions, the overall number of opposing frames cited in testimonies for HB 3112 decreased by almost 50%. Fewer people brought up the risks of public consumption of cannabis associated with exposure to secondhand smoke, driving under the influence of cannabis, and impacts to youth and mental health. The opposition instead shifted to application of the racial equity lens.
Bridging the Gap: Targeted Universalism
One testimony in support of HB 3112 leveraged language that invoked targeted universalism. It focused on how centering the needs of the few facing the highest barriers to entering the industry can in turn benefit everyone, such as directing tax revenue to historically marginalized communities. Cultivating this lens and policy approach can help bridge the gap and show the benefits of leading with a racial equity lens, as well as address unintended consequences from public consumption policy, like road safety and youth impacts.
“Furthermore, investment of much-needed resources into programs that rebuild wealth for the Black and brown communities decimated by the Drug War is a worthy use of cannabis tax revenue. These investments in education, home ownership, business development, and job training, will benefit all Oregonians.”
For the results from the testimony framing analysis in full detail, see Appendix II.
Assessment Summary
Table 8 outlines the expected direction, likelihood, severity, and magnitude of changes resulting from public consumption of cannabis. Table 9 provides a legend to interpret Table 8.
All changes derive from the direct increase in public places to consume cannabis that would be created, and the continued normalization of cannabis that would be advanced. Positive changes are primarily those brought by increased cannabis sales, jobs, and tax revenue. Available evidence suggests small, if any, changes to housing stability, academic achievement, and employment. Public consumption policy is expected to result in negative changes in youth use, crash risk, respiratory health, and mental health.
| Expected Impacts | Direction | Likelihood | Severity | Magnitude | Distribution (Equity Impacts) | Nature of Change |
|---|---|---|---|---|---|---|
| Cannabis Sales + Tax Revenue | STK – Increase LR – Increase FA – Increase | Highly Likely | Limited | Limited | Restorative Equity Effects through equity licenses | Nature of Change |
| Employment | STK – Decrease LR – Increase FA – Increase | Not Likely | Limited | Limited | Limited | Mixed or Unclear |
| Housing Stability | STK – Mixed LR – Limited FA - Increase | Not Likely | Limited | Limited | Restorative Equity Effects for low-income renters | Mixed or Unclear |
| Academic Achievement | STK – Decrease LR – Mixed FA – Limited | Not Likely | Limited | Limited | Limited | Mixed or Unclear |
| Adult Recreational Use | STK – Increase LR – Limited FA – Limited | Somewhat Likely | Low | Limited | Limited | Mixed or Unclear |
| Youth Use | STK – Increase LR – Increase FA – Increase | Moderately Likely | High | Medium | Disproportionate Harms | Mixed or Unclear |
| Crash Risk | STK – Increase LR – Increase FA – Increase | Moderately Likely | High | Limited | Limited | Majority Negative |
| Poor Respiratory Health Outcomes | STK – Increase LR – Increase FA – Increase | Moderately Likely | Medium | Medium | Disproportionate Harms | Majority Negative |
| Poor Mental Health Outcomes | STK – Increase LR – Mixed FA – Mixed | Somewhat Likely | High | Medium | Disproportionate Harms | Majority Negative |
| Assessment Category | Description |
|---|---|
Direction Will the outcome increase in its quantity or rate, decrease, or remain the same? | STK – Stakeholder Interview results LR – Literature Review results FA – Framing Analysis results Increase – The policy would increase the impact Decrease – The policy would decrease the impact Mixed – Evidence exists to support both increases and decreases of the impact Limited – There is not enough evidence to support a conclusion |
Likelihood How certain is it that the decision will affect health determinants? | Not Likely – The probability this will occur is very small, evidence exists against the mechanism of effect Somewhat Likely – The probability this will occur is small, limited supporting evidence Moderately Likely – The impact is relatively likely to occur, consistent supporting evidence exists Highly Likely – The impact has a high probability of occurring, with substantial supporting evidence Limited – There is not enough evidence to support a conclusion |
Severity How important is the effect on human health and well-being? | Low – The nature of the impacts result in limited or reversible effects on health Medium – The nature of the impacts results in chronic, substantial, but manageable effects on health High – The nature of the impacts are potentially disabling or life threatening Limited – There is not enough evidence to support a conclusion |
Magnitude How much will outcomes change because of the decision? | Low – Causes impacts to no or few people Medium – Causes impacts to a wider number of people High – Causes impacts to many people Limited – There is not enough evidence to support a conclusion |
Distribution Will the effects be distributed equitably across populations? | Expected subpopulations are described. Disproportionate Harms – The policy will result in disproportionate adverse effects on subpopulations Disproportionate Benefits – The policy will result in disproportionate beneficial effects on subpopulations Restorative Equity Effects – The policy will rectify existing disparities Limited – There is not enough evidence to support a conclusion |
Nature of Change Are the effects positive, negative, or unclear? | Majority Positive Majority Negative Mixed or Unclear |
Characterizations adapted from: Bhatia R. Health Impact Assessment: A Guide for Practice. Oakland, CA: Human Impact Partners, 2011 and Rhodus et al. A review of Health Impact Assessments in the U.S.: Current State of Science, Best Practices, and Areas for Improvement. EPA, 2013.
Recommendations
Linking Impacts with Action
There are opportunities to mitigate harms and maximize benefits if cannabis becomes lawful to consume in public venues. The mitigation actions below focus on limiting youth initiation of cannabis use, reducing cannabis smoke exposure, promoting safe driving, minimizing mental health impacts and incorporating an equity lens into county perspectives on cannabis.
| Category | Impacts | Actions |
|---|---|---|
| Social | Cannabis-related employment and tax revenue are likely to increase in light of legislation. | Direct increasing cannabis tax revenue to address disproportionate harms created or made worse by public consumption. |
| Social | Clackamas County youth rates of cannabis use have held steady over the past years, but the state overall has seen continued increase in use. It is possible that youth use would increase through increased exposure and normalization. | Increase awareness of the negative effects of cannabis on youth and take action to prevent youth initiation. |
| Social | The creation of destinations for public consumption of cannabis will have local, site-specific impacts in both urban and rural areas that will affect safety and livability. | Craft zoning policy to promote health and well-being through the built environment. |
| Health | Mental health conditions can be exacerbated through heavy cannabis use. | Address the role of cannabis in mental health outcomes and craft policies and programs to address them. |
| Health | Toxic air pollutants from cannabis smoke, as well as secondhand exposure, can lead to negative health effects. | Protect and maintain the Indoor Clean Air Act to ensure all Oregonians are protected from secondhand smoke. |
| Health | More people will drive under the influence of cannabis due to an increased number of public locations to consume cannabis, and the dispersed, rural nature of the county. | Adopt a Safe System Approach that lowers speed limits, addresses upstream interventions to reduce driver substance consumption, and prioritizes community engagement and education. Continue to offer in-class high school presentations to address risks of driving and substance consumption. Build new microtargeted campaigns to address driving and substance consumption. |
| Equity | If increased cannabis use follows historic trends, public consumption allowance will not result in equitable distribution of cannabis access or health outcomes. | Adopt a Safe System Approach that lowers speed limits, addresses upstream interventions to reduce driver substance consumption, and prioritizes community engagement and education. Continue to offer in-class high school presentations to address risks of driving and substance consumption. Build new microtargeted campaigns to address driving and substance consumption. |
| Equity | The topic of equity was notably absent in stakeholder interviews. | Promote discussion and community capacity building around cannabis and racial equity. |
Recommendations
Recommendations are primarily for stakeholders and decision-makers across the sectors that intersect with cannabis use. This includes county and city elected officials, agencies responsible for implementation of cannabis regulation, and health and community advocates. They may also apply to other local county jurisdictions in Oregon, especially those with rural communities.
- Support and increase health equity-focused advocacy in cannabis policy development as legislation is being shaped. There was a lack of health-focused advocacy in the 2021 legislative session. Considerations and steps for implementation include:
- Ensure general health equity outcomes and considerations are cited in policy development as a foundational need. While HB 3112 highlights economic and social justice needs, the bill introduction does not include background or context regarding health disparities or cannabis access. Including this language in policy development provides an important framework for stakeholders and decision-makers to evaluate policy after implementation.
- Invest time and energy into cross-sector coalition building. The benefits and burdens perceived were starkly different between sectors. Building cross-sector partnerships and intentionally identifying shared goals will better support the development of health-promoting cannabis policy.
- Provide technical assistance and support to youth, mental health advocates, and health organizations to participate in the legislative process. These voices were notably absent from the 2021 testimony participants. Personal stories and authentic voices are powerful. Technical assistance could take the form of data provision or assistance navigating the legislative process.
- Advocate for rural needs. There was a lack of rural representation in testimonies submitted during the legislative hearings, and rural areas will experience the effects of public consumption policy different than urban areas. Grow sites will likely experience more traffic should consumption be permitted in farm tourism events.
- Adopt local regulations and zoning requirements to reduce the impact of public consumption of cannabis on neighborhood health. Health-promoting policies need to intentionally shape the indoor and outdoor built environment to support healthy communities. Growing evaluation of public consumption policies at the local level show a wide spectrum of regulations addressing secondhand smoke and clean air, not all of which fully protect health.9 Additionally, marketing and visible access in neighborhoods influence use, and in turn health. For example, studies show that increased accessibility to alcohol and tobacco retail stores leads to an increase in use, and the density and proximity of tobacco retailers to schools affects youth tobacco rates. Increased tobacco retailer density is associated with experimental smoking, and the prevalence of smoking has been shown to be higher at schools with five or more retailers in the area.51, 52
- Incorporate health protective design, operation, and building code features. The most effective way to reduce exposure to secondhand cannabis smoke is to establish public consumption policy that bans cannabis smoking or vaping indoors, and only permits edible consumption indoors. Establishing strict requirements and design features for outdoor consumption spaces (inclusion of visual barriers such as non-permeable fencing, tree plantings, etc.) will aid in reducing visual exposure and protecting clean indoor air.
- Limit public consumption permits to standalone buildings. This requirement would create a balance of allowing on-site consumption while protecting employee health, providing opportunity for consumption monitoring, and minimizing impacts on neighboring residences or businesses.53 Should outdoor consumption of cannabis occur in mixed-use buildings, cannabis smoke may affect neighboring businesses or residences. This is a current impact of tobacco smoke in the county.
- Evaluate and adopt zoning and licensing policies that reduce the number and proximity of public consumption locations to schools, parks, and churches. Existing cannabis retail regulations in the county already provide strict development standards and requirements. Public consumption licensing needs to follow similar, if not stricter, regulations. Spatial analysis evaluating zoning, demographics, and current land use can inform specific recommendations for code to avoid unanticipated and unwanted impacts in communities. Regulations that protect areas where children recreate (playgrounds, schools, and daycares) should be prioritized.
- Regulate marketing and advertisement of public consumption sites. Studies on exposure to tobacco and alcohol marketing show an association between lower perceived risk and higher use with youth. Youth in Oregon report common exposure to cannabis advertisements already.54 Local regulations should be implemented following OHA guidelines and recommendations. These could include the maximum size and number of signs per location/event. Additionally, educational signs including health information, effects of cannabis use, and risk of overconsumption should be explored and codified.
- Develop an equity lens to guide the development and evaluation of cannabis use and regulation. Policies should consider communities disproportionately and negatively impacted by issues associated with substance use and other related health harms. In addition to harms caused by over-policing and racial profiling, the stigmatization of cannabis has also disproportionately impacted communities of color. The topic of equity was notably absent in stakeholder interviews, with concerns about disproportionate impacts only surfacing in three of 24 interviews. Invest in understanding the equity implications in housing, economic development, and health access. Considerations and steps for implementation include:
- Develop targeted universalism framing to discuss cannabis equity. Targeted universalism is a policy approach that involves setting universal goals for the general population and using targeted, specific strategies for sub-populations based on context and need.55 It is a methodology that works to address disparities. Shaping policy with this lens can help build support with groups who may feel left out.
- Collaborate with other equity advocates to initiate conversations that center race. Equity advocates are critical partners to include when evaluating policy options.
- Co-create the equity lens through conversations with local community-based organizations and communities of color. Policy informed with the lived experiences of community members better serves their needs, builds trust in local government, and increases community empowerment and resilience.
- Dedicate funding and resources for systems to promote safety and limit driving under the influence of cannabis. Current Clackamas County zoning code prohibits cannabis retail within 1500ft of light rail stations, which encourages users to drive to and from possible future public consumption sites. Transit stops within 400m of start or end destinations are significantly more likely to be used. Transit coverage in Clackamas County, while growing under guidance of the Transit Development Plan, still has significant service gaps. These conditions create an environment where people in the county will be much more likely to drive to a destination to consume cannabis rather than walk or use a ride share service, taxi, or public transit. Given a growing number of crashes involve some form of substance, additional safety efforts are needed. Considerations and steps for implementation include:
- Implement best practices from early public consumption adopters. Jurisdictions around the U.S. that have implemented public consumption policies have adopted a variety of measures to promote safety. These include barring the consumption and sale of alcohol and tobacco on site, prohibiting employees from consuming cannabis while working, and monitoring consumer behavior to avoid overconsumption and community disturbances.
- Develop and implement consumption monitoring standards and training for bud tenders and event staff. Training should cover impacts of cannabis use, current laws and regulations, past and current inequities in cannabis use and trauma-informed de-escalation practices. Training should be developed with an equity lens and co-created with community members.
- Support ride service and transit access near public consumption locations. Free or discounted rides can be offered at consumption sites to reduce patrons’ likelihood of operating a vehicle under the influence. Transportation options should be considered in event planning where public consumption will be allowed and evaluated in the permitting process. As local governments develop zoning regulations, they should consider access to public transit as it relates to public consumption locations and event spaces.
- Develop public information materials on lower risk cannabis use, cannabis consumption types, and the impacts of secondhand cannabis smoke exposure. As cannabis normalization and use continue to grow, so too must related health and safety education and awareness efforts. Considerations for implementation include:
- Underscore the health risks of any inhalable substance while decoupling from the broad category of cannabis. Focusing on the risks of particulate matter inhalation, regardless of source, provides a more objective advocacy platform as the research develops on full health effects. Evidence supports that cannabis use has therapeutic effects for some conditions when dosed correctly. Cannabis edibles offer an alternative to smoking or vaping cannabis. Edible consumption reduces the risk of poor respiratory health outcomes associated with smoking, but does not address other concerns, such as road safety.
- Include lockbox information and safe storage. Encourage adults to lock and securely store cannabis products at home to prevent children and youth from consuming them.
- Identify distribution points for cannabis informational materials. Potential sites to distribute educational materials include licensed public consumption venues and events. Develop an event toolbox and training guide for staff and reserve space at events with public consumption to share educational materials and lock boxes.
- Incorporate cultural awareness and multilingual information. Effective messaging needs to be culturally tailored and co-developed with community partners. Use clear, plain language with pictorial warnings, and make messages available in multiple languages.
- Partner with health care workers and educators. Expand the reach of cannabis education by collaborating with health care clinics, particularly federally qualified health care centers and schools. Building staff capacity and training on the health impacts of cannabis, including current research and policy around cannabis, can then be passed on to patients, students and parents. Continue to partner to present to high school students on the risks of public consumption and risk taking.
- Continue to develop and implement behavioral change campaigns focused on driving and cannabis consumption. The Department of Transportation and Development Traffic Safety Program leverages the Positive Culture Framework to encourage safe road behavior. This framework could be applied in the continued development of campaigns around cannabis consumption, such as designating drivers when traveling to public consumption venues.
- Create strong accountability mechanisms to ensure benefits to historically marginalized groups are maintained for the lifespan of public consumption policy. In the 2021 HB 3112 legislation, specific policy provisions were designed to address the past harms that have fallen on communities of color related to cannabis consumption and the War on Drugs. Methods of repairing generational harms require long-term monitoring and accountability to ensure they don’t fall by the wayside. Related to public consumption, licenses exclusive to BIPOC business owners were provisioned, but set to become available to all after 10 years of implementation.
- Create an evaluation plan to monitor unintentional consequences. The evaluation plan should center communities of color and include the voices of diverse stakeholders that intersect with the cannabis industry and provide transparency into program impact. The sectors interviewed for this HIA could serve as a starting point for recruitment and should extend to equity-license holders. The evaluation should include equity, health and safety impacts as well as new challenges that occur in implementation.
- Mandate the Equity Oversight Board to review health and access disparities. Draft legislation in 2021 charged this board with establishing key performance indicators related to cannabis equity. There should also be a formal charge to include cannabis-related health and safety indicators. They should include insight into mental health, youth use, road safety, and rural impacts.
- Advocate for the use of cannabis tax revenue for local interventions to support livability and reduce unintended impacts on the surrounding area. Creating destinations where cannabis can be consumed creates new community exposures to cannabis. Neighborhoods with higher densities of low-income and BIPOC communities are at risk of being disproportionately saturated with venues allowing public consumption. This is a common trend with tobacco and alcohol outlets.
- Establish partnerships with local researchers to support the translation of evidence to practice and advocate for research in rural settings. Research on the relationship between cannabis use and health outcomes is limited in the United States because of federal regulations and restrictions on both cannabis and research. Furthermore, existing research on cannabis rarely evaluates differences between cannabinoids (THC vs CBD), cannabis products, potencies, and modes of consumption. The evidence that has been generated often concludes in mixed outcomes. For this reason, it is important to ask questions about the benefits and harms of cannabis use, and for whom.56 Developing local relationships with research partners that operate within the same policy conditions is key to developing relevant and actionable evidence. Possible research topics include:
- Economic assessment study of cannabis at the county level to understand trends in sales, revenue, job creation, and effects in other sectors
- Evaluation of distribution of public consumption sites and events against demographic information and other social determinants of health
- Distinguish the differences in urban, suburban, and rural impacts
- Monitor health-related outcomes like cannabis-use disorder, cannabis-related emergency department visits, and cannabis-related crashes
Addendum
2023 Legislative Session
The attempt to pass public consumption of cannabis policy was revisited in Oregon’s 2023 legislative session. An amendment to House Bill 2516 would have permitted cannabis producers to operate a “cannabis tourism center” on their property, allowing tours of production facilities, educational activities, marketing, and the sale cannabis products processed by the producer. It also would have allowed the sampling of usable marijuana products.
Language in the bill set the sampling limit at 3.5 grams of usable marijuana per patron per day. (Pre-rolled joints at Oregon cannabis retailers typically contain one gram of usable marijuana each.) House Bill 2516 offered little to protect the health and safety of tourism center employees exposed to secondhand smoke or communities that may, due to these facilities’ proximity, see increased instances of impaired driving. However, language in the bill appeared to keep the centers from violating Oregon’s Indoor Clean Air Act.57
Although the bill moved out of committee with bipartisan support, it did not progress any further due to a walkout by legislators that ultimately ended the prospects of hundreds of pieces of legislation.58
Endnotes
1 National Conference of State Legislatures. Cannabis Overview. 2022.
2 National Conference of State Legislatures. State Medical Cannabis Laws. 2023.
3 Pew Research Center. Two-thirds of Americans support marijuana legalization. 2019.
4 Oregon Behavioral Risk Factors Surveillance System. Adult Prevalence Data. 2018-2021.
7 OpenSecrets. Industry Profile: Marijuana. 2019.
8 Gourdet, C., Gagnon, F., Moscetti, C., Obradovic, I. Regulating Private and Public Places of Non-Medical Cannabis Consumption in North America: Public Health and Public Safety Issues. Journal of Canadian Studies. 55(2) p. 279-306. 2021.
10 Oregon NORML. New Revenue Coalition Formed to Create Social Cannabis Consumption Spaces in 2019.
11 Oregon Legislative Assembly. House Bill 2233. 2019.
12 Oregon Nurses Association. Report on the 2019 Oregon Legislative Session. 2019 (PDF)
13 City of Portland. City of Portland 2019 Legislative Report. 2019
15 Oregon Legislative Assembly. House Bill 3112. 2021.
16 Conduent Healthy Communities Institute. Demographics: Clackamas. Blueprint: For A Healthy Clackamas County. Accessed 4/23/2023.
18 Oregon Health Authority. Youth marijuana use, attitudes and related behaviors in Oregon. 2019 (PDF).
19 Oregon Secretary of State. Voters’ pamphlet. 1998.
20 Oregon Department of Revenue. Oregon Marijuana Tax: Distribution Information. 2022 (PDF).
21 Oregon Office of Economic Analysis. Oregon Economic and Revenue Forecast. March 2023 (PDF)
22 Oregon Cannabis Commission. Oregon Cannabis Commission Report. 2019 (PDF)
27 Cannabis Liberalization In The US: The Policy Landscape, Health Affairs Health Policy Brief, July 1, 2021. DOI: 10.1377/hpb20210518.36548.
28 Schauer GL, Njai R, Grant-Lenzy AM. Modes of marijuana use - smoking, vaping, eating, and dabbing: Results from the 2016 BRFSS in 12 States. Drug Alcohol Depend. 2020 Apr 1;209:107900. doi: 10.1016/j.drugalcdep.2020.107900. Epub 2020 Feb 6. PMID: 32061947.
29 Romm KF, West CD, Berg CJ. Mode of Marijuana Use among Young Adults: Perceptions, Use Profiles, and Future Use. Subst Use Misuse. 2021;56(12):1765-1775. doi: 10.1080/10826084.2021.1949724. Epub 2021 Jul 22. PMID: 34294001; PMCID: PMC8693385.
31 Cerdá M, Wall M, Feng T, et al. Association of State Recreational Marijuana Laws With Adolescent Marijuana Use. JAMA Pediatr. 2017;171(2):142–149. doi:10.1001/jamapediatrics.2016.3624.
32 Environmental Protection Agency. Indoor Particulate Matter. Accessed 10/18/21.
34 Environmental Protect Agency. Particulate Matter (PM) Basics. Accessed 5/1/23.
36 Murphy M B, Huang A S, Schik S F. PM2.5 Concentrations in a Cannabis Store with On-Site Consumption. Environmental Health Perspectives, 2021. 129(6), p. 2-3.
37 ASHRAE. ASHRAE Position Document on Environmental Tobacco Smoke. 2020 (PDF)
39 Center for Health and Safety Culture. Key Information for Cannabis and DUIC Policy. 2019 (PDF)
40 Oregon Revised Statutes § 813.010 (1983 and rev. 1985, 1987, 1991, 1999, 2003, 2007, 2009).
42 Clackamas County. Drive to Zero Safety Action Plan. 2019.
43 McCaffrey D.F, et al. Marijuana Use and High school Dropout: The Influence of Unobservables. Health Economics, 2010. 19(11) p. 1281-1299.
44 National Institute on Drug Abuse. Cannabis (Marijuana) Research Report. 2020.
45 Biasutti W R, Leffers K S H, Callaghan R C. Systematic Review of Cannabis Use and Risk of Occupational Injury. Subst Use Misuse. 2020;55(11):1733-1745. doi: 10.1080/10826084.2020.1759643. Epub 2020 May 22. PMID: 32441179.
46 Sabia J, Nguyen T T. The Effect of Medical Marijuana Laws on Labor Market Outcomes. The Journal of Law & Economics, 2018. 61(3) p. 361-396.
48 Mid-Atlantic ADA Center. Medical Marijuana and The ADA. 2020 (PDF)
50 Berkeley Media Studies Group. Framing 101. Accessed 5/1/23.
51 Henriksen L, Feighery E C, Schleicher N C, Cowling D W, Kline R S, Fortmann S P. Is adolescent smoking related to the density and proximity of tobacco outlets and retail cigarette advertising near schools? Prev Med. 2008 Aug;47(2):210-4. doi: 10.1016/j.ypmed.2008.04.008. Epub 2008 Apr 29. PMID: 18544462.
53 Steinberg J, Unger JB, Hallett C, Williams E, Baezconde-Garbanati L, Cousineau MR. A Tobacco Control Framework for Regulating Public Consumption of Cannabis: Multistate Analysis and Policy Implications. Am J Public Health. 2020 Feb;110(2):203-208. doi: 10.2105/AJPH.2019.305423. Epub 2019 Dec 19. PMID: 31855488; PMCID: PMC6951385.
56 Cousijn J, Núñez A E, Filbey F M. Time to acknowledge the mixed effects of cannabis on health: a summary and critical review of the NASEM 2017 report on the health effects of cannabis and cannabinoids. Addiction. 2018 May;113(5):958-966. doi: 10.1111/add.14084. Epub 2017 Dec 21. PMID: 29271031; PMCID: PMC9520128.
57 Oregon Legislative Assembly. 2023 Session.
58 Oregon Legislative Assembly. 2023 Session.
59 The Network for Public Health Law. Cannabis Regulation Fact Sheet. 2022 (PDF)
61 Oregon Medical Marijuana Program. Statistical Snapshot: July 2021. 2021. (PDF)
62 Oregon Liquor and Cannabis Commission. Minor Decoy Operations. 2023.
63 Oregon Liquor and Cannabis Commission. Marijuana Business Licenses Approved. 2022.
64 Oregon Health Authority. 2020 Oregon Student Health Survey (PDF)
65 Oregon Health Authority. 2022 Student Health Survey (SHS) School Summary Results (PDF)
66 Oregon Health Authority. 2018 Oregon Student Health Survey (PDF)
